Explanation
Learning objectives Understand
Explanation
Head and neck cancer is a generic term for cancers that develop in the neck or upper parts of the body, excluding the brain. In this area of the body, various organs are located anatomically closely to each other and each has important functions.
Operable tumors, even in advanced stages, have high 5-year survival rates (eg. the 5-year survival rate of stage III/IV advanced tongue cancer is above 50%). Therefore, multidisciplinary treatments (surgery + radiotherapy + chemotherapy) are often used with curative intent. Any post-treatment disorders should be managed adequately to ensure that cancer survivors can live functionally with good QOL.
Among head and neck tumors, squamous cell carcinoma is the most common histological type and highly sensitive to radiotherapy and chemotherapy. For this reason, some patients avoid surgical options and instead chose to receive chemoradiotherapy as an organ-preserving treatment option. Surgical options include reduction surgery and reconstruction procedures that have been developed for better preservation of function.
Explanation
Patients with dysphagia caused by cancer treatment or by the cancer itself also need to accept the fact that they are "cancer" patients. Even during rehabilitation, many patients are anxious about survival and are scared of recurrence. Pain or slight changes experienced during swallowing training can trigger anxiety about recurrence. For the proper management of dysphagia, the condition can be classified into 3 types based on its cause-from surgery, radiotherapy, or the tumor itself.
Explanation
Dysphagia caused by radiotherapy
Irradiation to the head and neck region can have substantial effects on swallowing function. Because the severity of the disorder varies depending on the extent and dose of irradiation received, we should check the details of radiotherapy treatment that the patient received. For example, combined disorders of the following can lead to reduced swallowing function: salivary glands (salivary hyposecretion); tongue (taste disturbance); tongue, tongue base, and pharyngeal wall (muscle weakness); and larynx and pharynx (decreased sensation, hypoesthesia). Videofluoroscopy findings typically show significantly shorter oral/pharyngeal transit time and percent residue. The concomitant use of antineoplastic agents synergistically improves treatment effects, leading to improved organ preservation and cure rates. Chemoradiotherapy is an effective organ-preserving option, but it is inevitably associated with the risk of dysphagia due to treatment-induced pain and mucositis. Gastrostomy may therefore be performed before chemoradiotherapy to ensure sufficient nutritional intake. However, being too dependent on gastrostomy feeding from an early stage of radiotherapy can lead to disuse syndrome, and severe muscle weakness caused by the irradiation may lead to dependence on gastrostomy feeding even after treatment is finished. So, it is important to try to maintain oral feeding as much as possible and to start rehabilitation before treatment.
Explanation
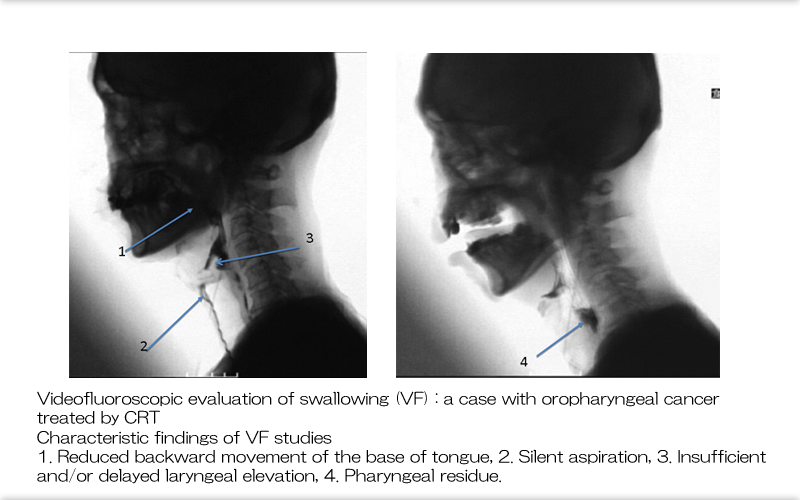
Dysphagia caused by radiotherapy
Here we see typical post-radiotherapy findings in VF studies. The findings include silent aspiration, aspiration due to delayed laryngeal elevation, and pharyngeal residue (pooling) due to reduced pharyngeal clearance.
Explanation
Characteristics of postoperative dysphagia
The characteristics of dysphagia caused by surgery include 1) being preoperatively predictable, 2) resection and reconstruction being the primary causes of anatomical changes, and 3) being influenced by pre- and postoperative radiotherapy and aging. An increasing number of elderly patients are receiving cancer therapy. In many cases, elderly patients before surgery can eat orally with no problems in nutritional intake or swallowing function. However, impairment of swallowing function related to aging may occur in the presence of certain stress factors, such as surgery and radiotherapy. It is also important to complete functional assessment before treatment starts.
Explanation
Dysphagia secondary to oral cavity cancer
Oral cavity cancer is variously referred to depending on the primary site. To develop an appropriate rehabilitation plan for dysphagia, we should know the effected site responsible for the dysfunction. It is particularly important to determine whether the hypoglossal nerve (tongue movement) and the mandibular branch of the facial nerve (lower lip movement) are preserved or not, as well as the extent of tongue resection. Bilateral damage to the suprahyoid muscles (eg. digastric muscle and geniohyoideus muscle) can lead to impaired elevation of the hyoid and larynx.
Explanation
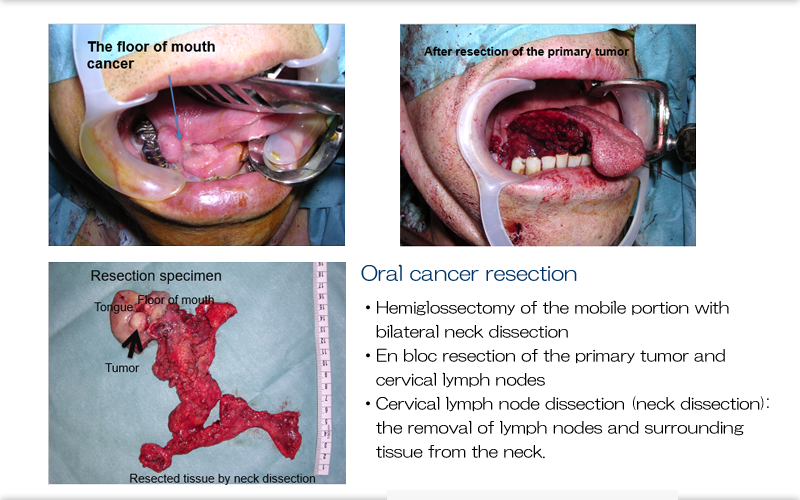
Operative field: Hemiglossectomy
Here we see the intraoperative findings for hemiglossectomy of the mobile tongue and neck dissection for cancer of the floor of the mouth. Postoperative functional impairment is caused by loss of function of the resected tissue, and accordingly, the manifestation of impairment varies depending on the extent and type of the tissue resected. We should therefore know the extent of resection of the mobile portion of the tongue, tongue base (anterior wall of the oropharynx), and mandible.
Explanation
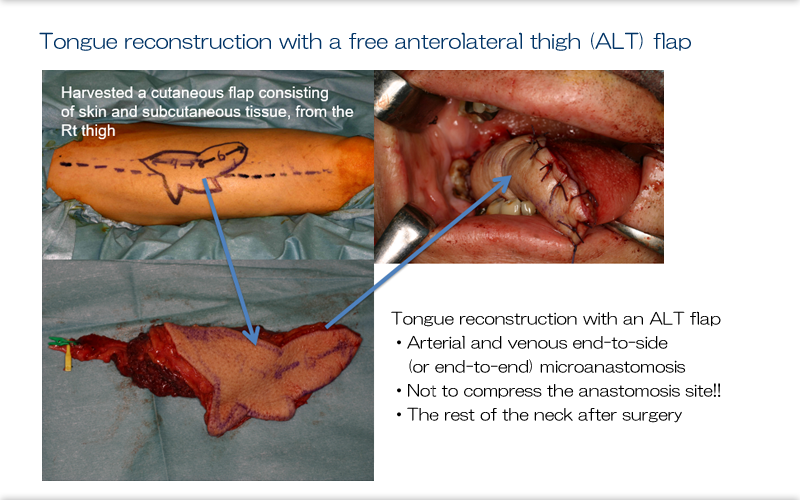
Free tissue transplantation
Tissue reconstruction with a free flap is an essential technique for the reconstruction of head and neck cancer. This slide continues on from slide 8 to show tongue reconstruction with a free anterolateral thigh flap. This patient has become able to eat a normal diet. Arteriovenous micro-anastomosis is performed in the neck. To ensure gentle handling of the peri-anastomotic area during postoperative management, the neck should be rested and the non-compressable site should be identified.
Explanation
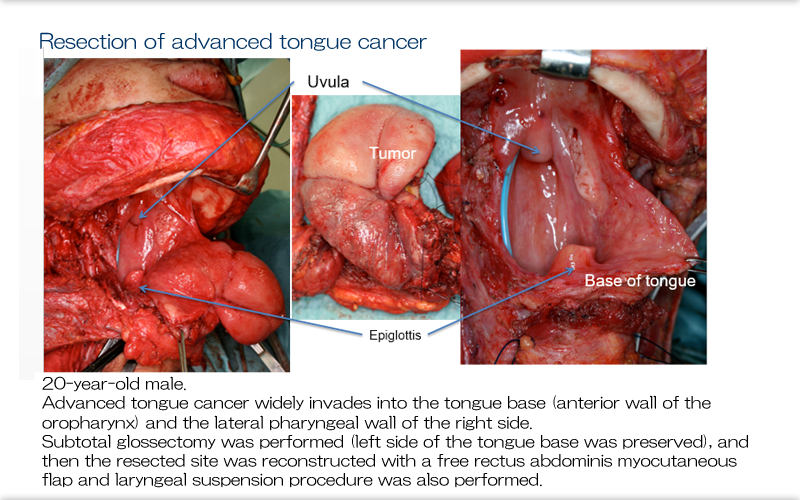
Resection of advanced tongue cancer
Extensive resection of the tongue base is the most important risk factor for dysphagia. In the case shown here, the tongue was reconstructed with a free rectus abdominis myocutaneous flap, in conjunction with cricopharyngeal myotomy and laryngeal suspension. The patient was discharged able to eat 100% rice gruel and later became able to eat katsudon (pork cutlet on rice), although the food needed to be cut into small pieces because of reduced masticatory force. No sign of recurrence has been noted for 12 years after surgery.
Explanation
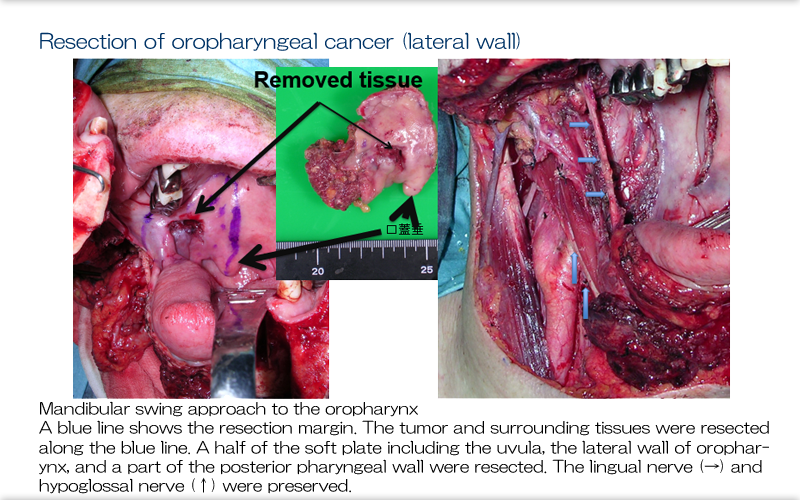
Resection of oropharyngeal cancer
Here we see the operative field for oropharyngeal cancer resection. The mandible is inverted, and the tongue base and oropharyngeal lateral wall are resected. After resection, the mandible is repositioned to the original position. The hypoglossal nerve or the superior laryngeal nerve may be resected depending on the extent of the tumor, which results in impaired tongue movement or reduced laryngeal sensation, respectively. This patient showed normal tongue movement with both nerves intact. The most common postoperative complications of oropharyngectomy are 1) velopharyngeal closure and 2) trismus.
Explanation
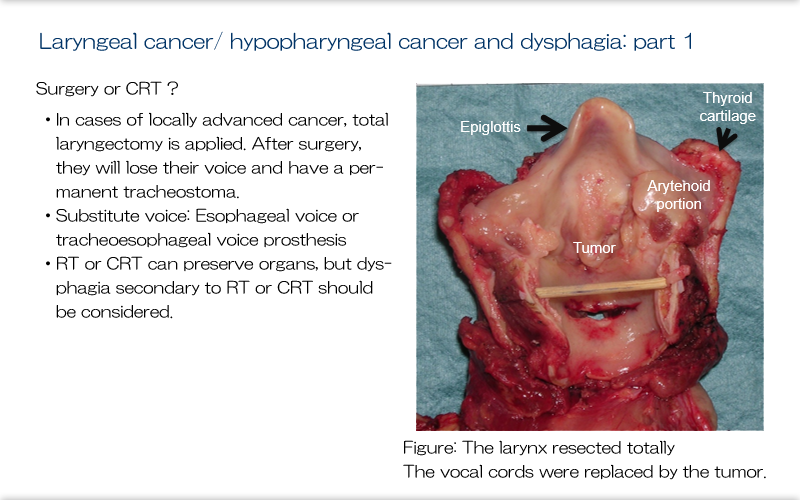
Treatment of laryngeal cancer/ hypopharyngeal cancer and dysphagia (1)
For laryngeal or hypopharyngeal cancer, the localization and/or stage of the lesion will determine the treatment strategies to use. For patients with advanced laryngeal or hypopharyngeal cancer, the problem is whether they can accept total laryngectomy, because it is associated with loss of vocal function and a permanent tracheostomy. It does, however, eliminate the risk of aspiration. Voice can be regained with voice training or additional surgery for speech support (TE shunt). Postoperative dysphagia after total laryngectomy can be caused by, but is not limited to, the following: 1) narrowing of the pharyngeal suture site or post-jejunal transplantation anastomotic stenosis, 2) velopharyngeal closure insufficiency after total laryngectomy in conjunction with extensive oropharyngeal wall resection, or 3) impaired bolus transport from the oral cavity due to combined resection of the hypoglossal nerve.
Explanation
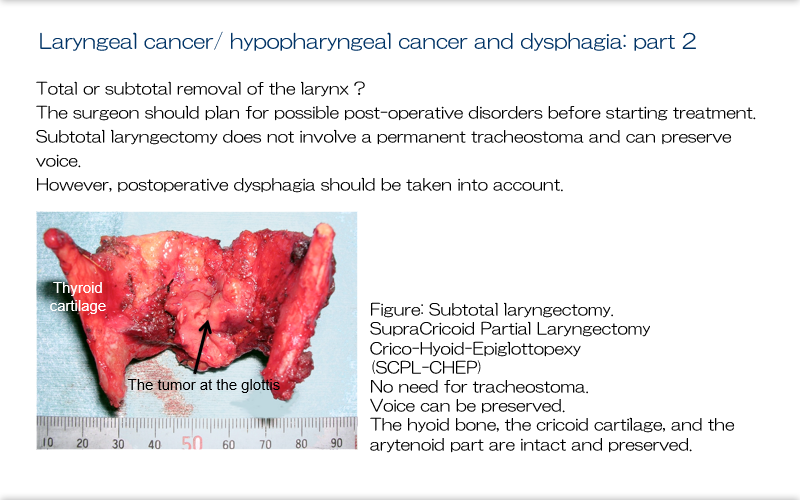
Laryngeal cancer: Treatment of hypopharyngeal cancer and dysphagia (2)
We see here a resected specimen from subtotal laryngectomy. This procedure is advantageous in that it does not involve a permanent tracheostoma, so voice is preserved, although care is still needed because of the risk of dysphagia. The surgeon should plan for possible post-operative disorders before starting treatment and obtain informed consent from the patient. Rehabilitation for these potential disorders should be started before treatment. Here we can see a specimen from supracricoid partial laryngectomy with cricohyoid-epiglottopexy (SCPL-CHEP). This procedure does not involve a permanent tracheostomy and so preserves voice. The hyoid bone/cricoid cartilage and arytenoid region are also preserved.
Explanation
Laryngeal cancer: Treatment of hypopharyngeal cancer and dysphagia (3)
In addition to the subtotal laryngectomy procedure shown on the previous slide, more variations are available for hemi- or subtotal laryngectomy procedures. The common characteristics of dysphagia caused by these procedures include 1) incomplete vocal cord closure, 2) limited laryngeal elevation, and 3) reduced laryngeal sensation. Postoperative training should be based on maneuvers aimed at improving laryngeal elevation, such as the Shaker exercise, and the supraglottic swallow to improve vocal cord closure. To improve posterior movement of the tongue base, as well as vocal cord closure, swallowing training such as focusing on the anchor point or tongue-hold swallow may also be effective. Patients who have undergone surgery for post-radiotherapy recurrence and elderly patients are more likely to have silent aspiration.
Explanation
Management of postoperative dysphagia
Before surgery, the extent of resection is determined and, based on this, the plan for reconstruction plan is developed. At this point, we can predict postoperative functional impairment to some extent, so informing the patients of training methods before the surgery allows for training to be introduced smoothly. Immediately after surgery, we need to prioritize the prevention of aspiration and safe management of the airway over swallowing training. The importance of oral care and pharyngeal hygiene remains the same during this stage. Before starting the training, functional assessment should be done to develop a plan for swallowing training. Training can start as soon as wound healing is achieved. Training should occur in steps according to the disease status and severity. Patients with a tracheostomy should also be encouraged to actively perform training.
References
- Logemann JA, Pauloski BR, Rademaker Aw, et al: Swallowing disorders in the first year after radiation and chemoradiation. Head Neck 30: 148-158, 2008,
- Ozawa K, Fujimoto Y, Nakashima T. Changes in laryngeal sensation evaluated with a new method before and after Radiotherapy. Eur Arch Otorhinolaryngol, 2009 Aug 25.
- Pauloski BR, Rademaker AW, Logemann JA, et al: Speech and swallowing in irradiated and nonirradiated postsurgical oral cancer patients Otolaryngology Head Neck Surg 118:616-24, 1998
- Salama JK, Stenson KM., List MA., et al: Characteristics Associated With Swallowing Changes After Concurrent Chemotherapy and Radiotherapy in Patients With Head and Neck Cancer. Arch Otolaryngology Head Neck Surg. 134(10):1060-1065.2008
- Fujimoto Y, Ozawa K, Ando a et al.: Dysphagia after treatment of oropharyngeal cancer. J. Jpn. Bronchoesophagol. Soc. 61(2), 2010
- Fujimoto Y, Nakajima T, Hasegawa Y: Prevention and management of dysphagia following surgery for head and neck cancer. JOHNS 19, 445-450, 2003
- Fujimoto Y, Nakajima T. Rehabilitation -Treatment of tongue cancer and articulatory/swallowing function-. MB ENT,70,61-69,2006
- Fujimoto Y, Hasegawa Y, Matsu-ura H, Nakayama B, Kato H: Swallowing function after curative resection and reconstruction of tongue cancer -Pathophysiology and management-. JOHNS, 16(4), 637-642, 2000
- Pauloski BA, Redemaker AW, Logemann JA, et al: Surgical variables affecting swallowing in patients treated for oral/ oropharyngeal cancer. Head Neck 26: 625-636, 2004
- Fujimoto Y, Hasegawa Y, Yamada H, et al. Swallowing Function Following Extensive Resection of Oral or Oropharyngeal Cancer With Laryngeal Suspension and Cricopharyngeal Myotomy. Laryngoscope, 117:1343-1348, 2007.
- Fujimoto Y, Iwata Y, Ozawa K, Ando A, Miyake M, Nakajima T: Functional outcomes after partial laryngectomy. The Larynx Japan 19(2), 70-74, 2007
- Mizojiri G and Kumakura I: Rehabilitation for Oral and Oropharyngeal Cancers. Ishiyaku Pub., Inc. 2000
- Asai M, Zenda S, Ota Y, Tahara M: Oral Care and Swallowing Rehabilitation to Support Chemoradiotherapy for Head and Neck Cancer. Oral Care, 2000