Explanation
The checking of vital signs is critical for risk avoidance. This module covers devices that are useful for this and can even be used by people who are not healthcare professionals. Suctioning techniques are also important to avoid aspiration and choking, so this module also covers suctioning techniques and suction machines.
Explanation
Checking of vital signs is fundamental to risk avoidance. The 4 main vital signs are body temperature, pulse rate, blood pressure, and respiratory rate.
This module discusses devices needed to measure these vital signs that are frequently used by dysphagia rehabilitation professionals across many different disciplines.
Previously, healthcare professional in only a few disciplines were permitted to directly suction sputum from patients. However, Japanese regulations were expanded in 2010 to allow therapists and clinical engineers to suction sputum as well (HPB Notification No. 0430(1), "Promotion of interdisciplinary team care through coordination and cooperation among different healthcare professionals", dated April 30, 2010). Professionals in other disciplines should still know general information about suctioning techniques because they may have to intervene in an emergency situation outside a medical facility.
Explanation
Body temperature typically refers to core body temperature, and axillary core body temperature is maintained in the range of 36.0°C. A temperature above 37.0°C is called a fever. A fever develops when inflammation-related endogenous pyrogens or toxins act on the body's thermoregulatory center. Therefore, fever is an important symptom of infectious diseases such as pneumonia. Accurate measurement of body temperature is critical because it can allow aspiration pneumonia to be detected early. So, patients' normal temperature should be measured routinely.
Explanation
As we see here, body temperature has physiological variabilities. The elderly typically have a low body temperature, and they are also less likely to develop a fever as an inflammatory response. So, exercise caution when comparing temperature measurements with normal temperature in this population.
Explanation
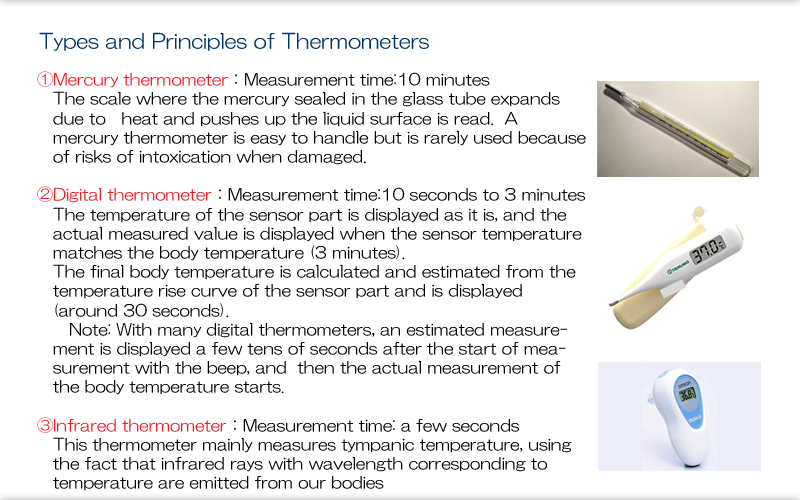
There are several types of thermometers available. Mercury thermometers are rarely used in modern medicine because they take too long to produce measurements, and because of their risks of intoxication when broken. Digital thermometers are mainly used. Digital thermometers measure temperature within approximately 30 seconds but provide an estimate rather than an actual measurement. They tend to give an inaccurate result when the thermometer is warm or there is a large difference between surface temperature and core body temperature. So, ensure that body temperature is measured in a normal room-temperature environment. Device performance also varies between products, and there is wide variation in pricing, but expensive thermometers are generally highly reliable. Infrared thermometers measure tympanic temperature. They can measure temperature in about 2 to 3 seconds and are considered more reliable than digital thermometers for repeated measurements. However, be aware that the thermometer will display a low temperature if the thermometer is very cold and cools down the tympanic membrane.
Explanation
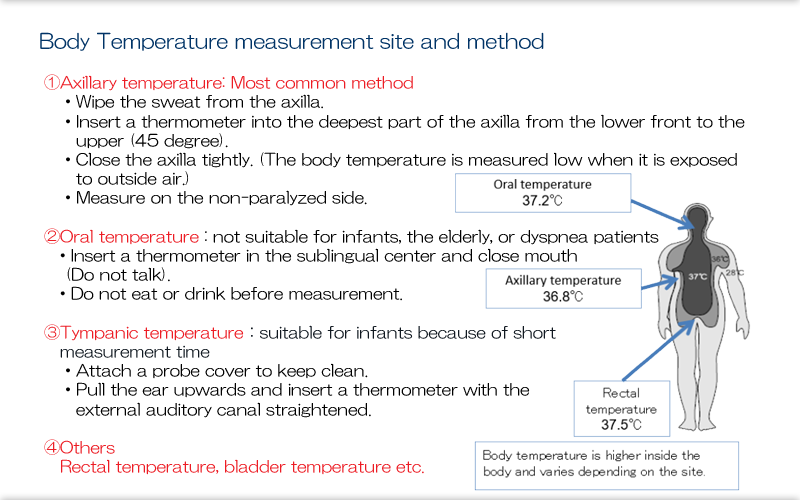
Here we can see different methods for measuring body temperature. Axillary body temperature is most commonly used, but make sure the armpit isn't wet and press the thermometer firmly against the skin. This is particularly important for patients who are thin-they need to press their arm tightly against their side.
Tympanic temperature is said to be higher than oral temperature but lower than rectal temperature. Make sure that the tympanic membrane is not covered with earwax before measuring tympanic temperature.
Explanation
A stethoscope is a device used to listen to sounds within the body. It is used for a wide variety of applications, from listening to physiological sounds such as the heart, lung, and bowel sounds, to listening for sounds that indicate disease such as heart murmurs, rales, chest congestion, and asthma sounds. Even with today's advanced diagnostic methods such as imaging tests and endoscopy, auscultation with a stethoscope continues to be a useful, simple, noninvasive, immediate, and repeatable method for evaluating a patient's condition. Auscultation of the neck, chest, and abdomen is frequently performed in dysphagia rehabilitation.
Even experienced doctors have considerable difficulty making an accurate diagnosis based on auscultation alone. But it is possible to learn how to identify abnormal sounds and to differentiate between right and left lung sounds by repeated listening, so even non-doctors should proactively try to use a stethoscope to see if they can notice any abnormalities.
Explanation
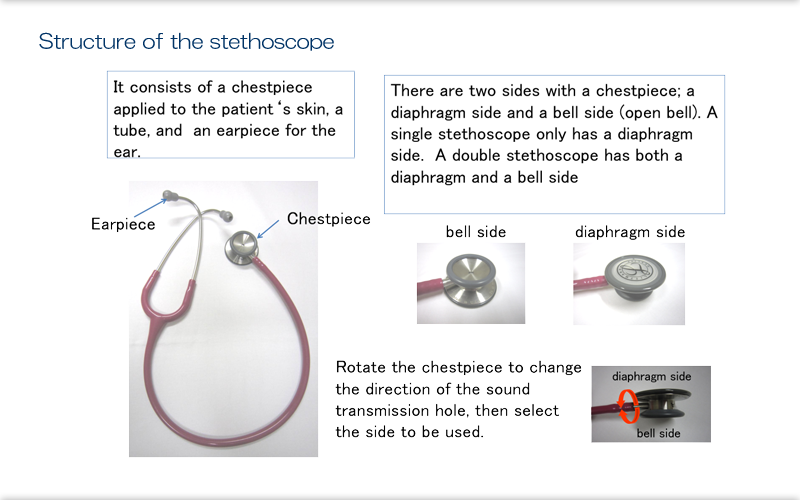
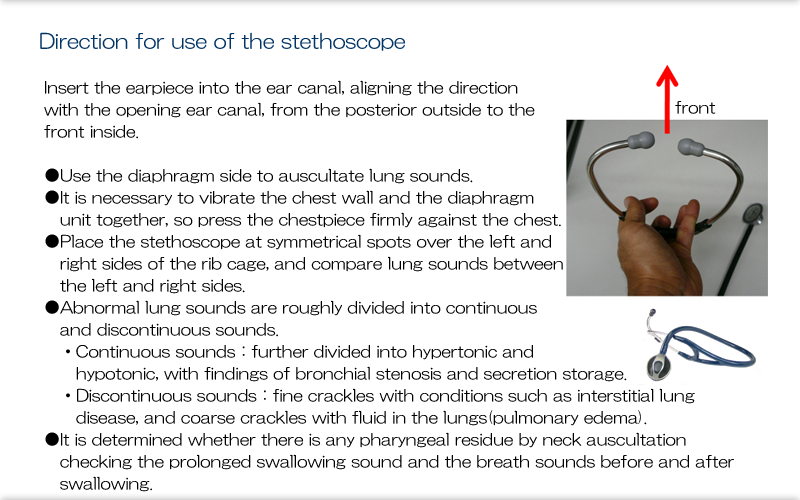
The most common type of stethoscope used has a bell side and a diaphragm side. The bell is designed to detect low-frequency sounds, and the diaphragm high-frequency sounds. These different uses are to help us differentiate between heart sounds, but only doctors really need to be aware of this. It is common to use the diaphragm only to listen for lung and bowel sounds.
Explanation
When inserting the stethoscope's earpieces, be aware of the direction that the stethoscope is facing.
When auscultating lung sounds, it is easy to identify abnormal sounds by positioning the stethoscope at symmetrical spots over the left and right sides of the rib cage and comparing lung sounds between the left and right sides. It is important to first listen to the lung sounds of healthy people to become familiar with normal lung sounds.
Abnormal lung sounds include louder or softer sounds as well as rales. These are breathing noises that can be heard with a stethoscope when certain abnormalities are present in the trachea, bronchi, or alveoli. The whistling and wheezing sounds heard in conditions such as asthma are called continuous sounds, and the bubbling sounds (coarse crackles) heard with fluid in the lungs (pulmonary edema) or bacterial pneumonia and crunching or crackling sounds (fine crackles) heard with conditions such as interstitial lung disease are called discontinuous sounds. Coarse crackles are also called moist rales, and dry sounds such as fine crackles are also called dry rales. Doctors often use these medical terms on patients' charts.
Refer to the section on other screening tests for neck auscultation.
Explanation
Blood pressure is the pressure exerted on arteries by contraction of the left ventricle. Pulse is measured at a peripheral artery from pulse waves produced by the beating of the heart. Both of these are vital signs. Blood pressure and pulse are indexes of circulation of blood through the body, and their measurement allows us to detect changes in circulation in a matter of seconds. A drop in blood pressure is directly life-threatening, so knowing a patient's blood pressure provides important information for risk avoidance-it allows care providers to quickly infer when a patient's condition is serious.
Normal blood pressure measured in an examination room is considered to be 140/80 or below, and anything higher is high blood pressure. There is no criterion for low blood pressure, but it can be detected by the appearance of symptoms such as dizziness at a systolic blood pressure of 80 mmHg or lower. Pulse is measured automatically using an automatic blood pressure monitor or pulse oximeter. Generally, a resting pulse of 60 or lower (called bradycardia) or 100 or higher (called tachycardia) is considered abnormal. Not only the rate but also the rhythm of the pulse is important. An abnormal rhythm is called an arrhythmia.
In exercise therapy for rehabilitation, there are criteria for whether or not a patient can exercise. The Anderson criteria, listed here for reference, illustrate the importance of measuring signs such as blood pressure and pulse.
● When to avoid exercise 1) Resting pulse rate ≥ 120 bpm 2) Diastolic blood pressure ≥ 120 3) Systolic blood pressure ≥ 200 4) Current exertional angina pectoris 5) Fresh myocardial infarction in the past month 6) Clear evidence of congestive heart failure 7) Marked arrhythmia other than atrial fibrillation 8) Palpitations and shortness of breath even before exercise
● When to stop exercise 1) Symptoms such as moderate dyspnea, dizziness, nausea, or anginal pain during exercise 2) Pulse exceeds 140 bpm during exercise 3) Ten or more premature ventricular contractions per minute, or arrhythmic tachycardia (eg, atrial fibrillation or supraventricular/ventricular tachycardia) or bradycardia, during exercise 4) Increase of ≥ 40 mmHg in systolic blood pressure or ≥ 20 mmHg in diastolic blood pressure during exercise
● When to temporarily stop exercise and resume after recovering 1) If the pulse rate increases by > 30% above the usual level during exercise and does not return to within 10% above the usual level after 2 minutes of rest, remaining exercise should be stopped or changed to very light exercise 2) Pulse rate exceeds 120 bpm 3) Fewer than 10 premature ventricular contractions per minute 4) Complaints of mild palpitations or shortness of breath
Explanation
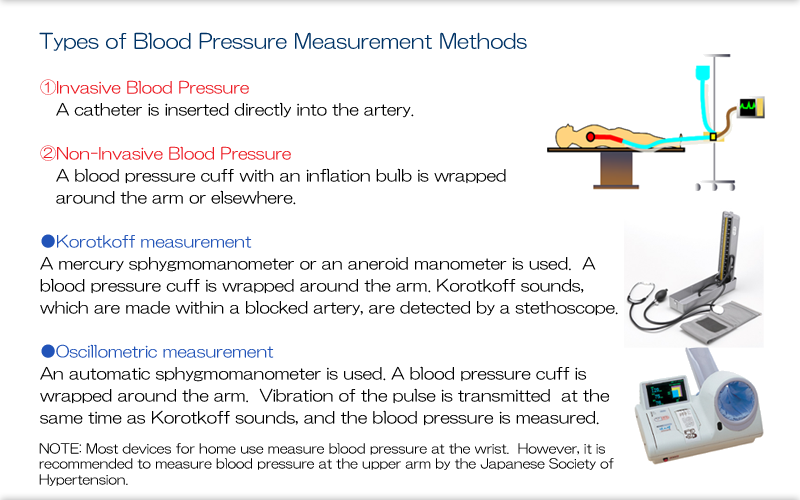
A catheter may be inserted directly into the artery, for example, during surgical procedures or in the intensive care unit.
Typically, a blood pressure cuff with an inflation bulb is wrapped around the arm or elsewhere, and air pressure is used to compress the artery. Blood pressure is measured from the difference between air pressure and arterial pressure.
Doctors and nurses can also measure blood pressure using a stethoscope, and automatic blood pressure monitors are now widely used as well. Oscillometric measurement produces reliable measurements regardless of the user's skill.
Most devices for home use measure blood pressure at the wrist. However, it is recommended to measure blood pressure at the upper arm in the elderly because measurement at a more central artery minimizes the effects of factors such as atherosclerosis.
Explanation
Here we see how to measure blood pressure using a cuff.
Ideally, the width of the cuff should match the size of the upper arm. However, there are few cuff varieties available, and they are mainly sized for adults or children. Consider using a children's cuff with highly emaciated patients.
The speed of depressurization is standard across automatic blood pressure monitors, but patients with bradycardia have a long interval between heartbeats, so the cuff must be depressurized slowly to obtain accurate measurements. Use a manual cuff with these patients.
Explanation
A pulse oximeter is a device that measures arterial oxygen saturation through the skin. The vital sign that it measures is called percutaneous arterial blood oxygen saturation (SpO2). Oxygen saturation measured in collected arterial blood is called SaO2.
Oxygen saturation shows what percentage of hemoglobin in red blood cells is bound to oxygen (ie, saturation).
It is one of the indexes of gas exchange, and it changes not only with lung problems but also with circulation problems, respiratory status, and atmospheric pressure.
In dysphagia rehabilitation, oxygen saturation is very important when evaluating changes in respiratory status due to choking or severe aspiration and when evaluating aspiration pneumonia.
Explanation
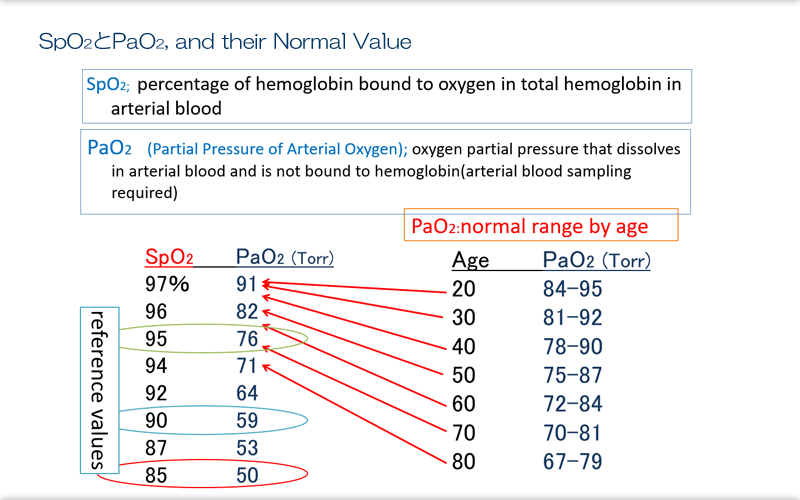
The normal value of SpO2 is ≥ 95%. SpO2 ≥ 90% is not greatly problematic clinically, but SpO2 < 85% is associated with impaired gas exchange in tissues.
Naturally, these are typical values when atmospheric pressure is 1 atm and oxygen concentration is 20%.
Oxygen does not dissolve easily in water, so hemoglobin binds to oxygen to transport it to peripheral sites. Oxygen that has entered the blood (plasma) by diffusion through the alveoli binds to hemoglobin. The amount of oxygen dissolved in plasma depends on pressure, and this pressure depends on atmospheric pressure. Oxygen concentration is about 20% at 1 atm of pressure, or about 760 Torr, which means that the partial pressure of oxygen in the atmosphere is about 150 Torr. At this pressure, oxygen passes through the alveolar walls and is pushed into arterial blood. Pressure decreases as the oxygen passes through the alveolar walls due to resistance, but there is little pressure loss in young people, whose alveolar walls are highly permeable, and pressure drops to only about 90 Torr. However, alveolar wall resistance and resulting pressure loss increase with age, which causes pressure to drop to about 70 Torr in elderly people. Various diseases can cause the alveolar walls to thicken, which increases pressure loss and reduces plasma oxygen pressure. When pressure drops, the amount of oxygen that can dissolve in plasma decreases.
When the partial pressure of oxygen is normal (about 90 Torr), oxygen saturation of hemoglobin is 97%, meaning that almost all oxygen is bound.
At peripheral sites, oxygen diffuses from plasma into tissue fluid and reaches cells of all types, at which point it is expended. The partial pressure of oxygen in tissue fluid is low, at 20 to 30 Torr, which allows for easy transfer of oxygen. Once oxygen is expended, the partial pressure of oxygen decreases by that amount. This decrease in the partial pressure of oxygen then causes oxygen that was bound to hemoglobin to separate from hemoglobin and enter the plasma. This oxygen moves into tissues. As a result, the partial pressure of oxygen in venous blood becomes about 40 Torr, and the oxygen returns to the lungs.
The partial pressure of oxygen (PaO2) in blood is fundamentally important in the transportation of oxygen to tissues, and the oxygen saturation of hemoglobin (SpO2) is widely used because it directly reflects PaO2, is non-invasive, and can be measured almost instantaneously.
On a side note, atmospheric pressure decreases by half at an altitude of 5500 meters. Under these conditions, PaO2 becomes 50 Torr, and SpO2 becomes 85%, which illustrates the harshness of the conditions at altitude.
Explanation
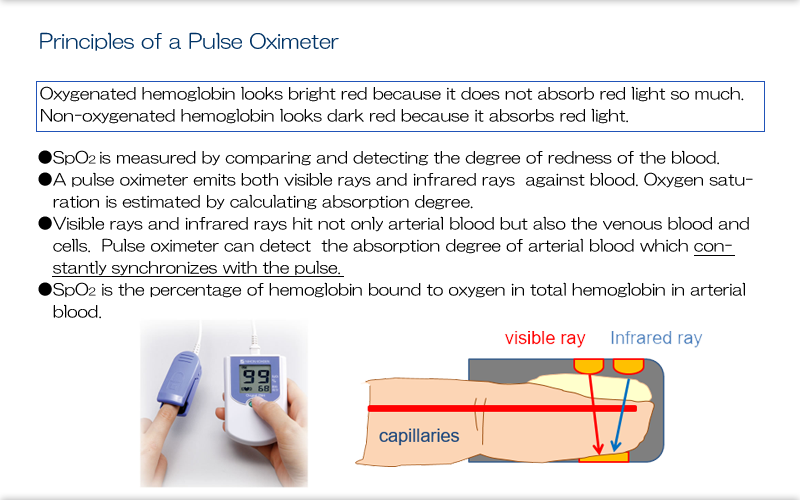
You may not need to understand how a pulse oximeter works in detail, but you should know that it measures saturation by emitting light waves into tissues, and that it detects arterial pulse and differentiates it from venous pulse.
You need to make sure that the sides of the probe (sensor) that emit and detect the light waves are perfectly aligned. Do not move or shake the probe. A certain amount of blood flow must be present for accurate measurement.
Explanation
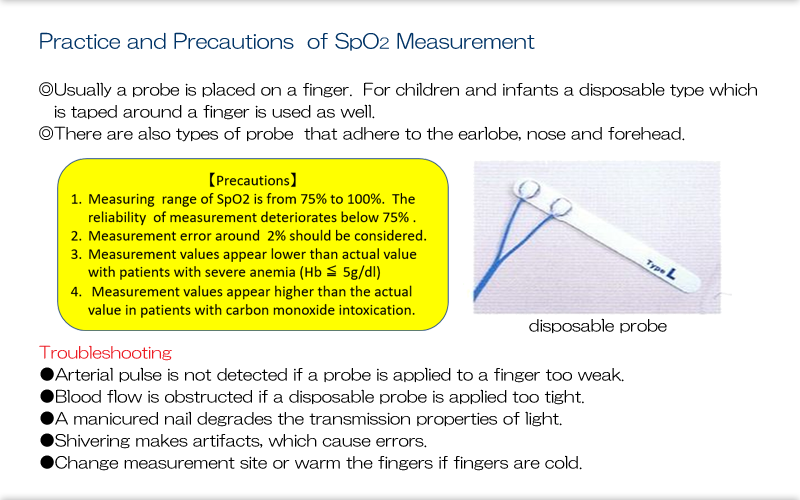
Here we see some precautions for using a pulse oximeter.
As mentioned earlier, the sensor parts must be perfectly aligned. The sensors of a finger pulse oximeter are always aligned, but with disposable sensors be aware that they sometimes must be carefully fitted to align with each other.
Explanation
Suctioning is performed for risk avoidance, and it is particularly important for avoiding emergency situations.
Professionals in only a limited number of disciplines are permitted to perform suctioning at medical facilities, but it is important that people working in dysphagia rehabilitation be prepared in case they encounter situations where they need to use suctioning techniques to avoid someone choking outside of a medical facility. Refer to the Suctioning Protocol published by the Japanese Physical Therapy Association.
The primary purpose of suctioning is to remove substances retained in the mouth and pharynx to prevent aspiration and choking. A catheter is inserted through the mouth or nose and advanced to the pharynx. The catheter cannot be inserted below the glottis, so airway secretions cannot be suctioned. Substances that have entered the pharynx through coughing or bronchial drainage are suctioned.
Regardless of what is being suctioned, the procedure stimulates the pharynx, which is uncomfortable and can induce vomiting. So, suctioning must be brief and well executed.
Endotracheal suctioning, which is done through an endotracheal tube, requires particular care due to the risk of tracheal injury, and it should not be done by a beginner. Refer to the Guidelines for Endotracheal Suctioning published by the Japanese Society of Respiratory Care Medicine.
There are various types of suction machines, but the most popular are the outlet type (installed on hospital walls) and the portable electric type. The manual type is designed for use in situations when electricity is not available, but it generally doesn't function well enough.
Low-pressure continuous suction machines that continuously suction saliva from the mouth are also available and can be useful for patients who aspirate saliva.
Explanation
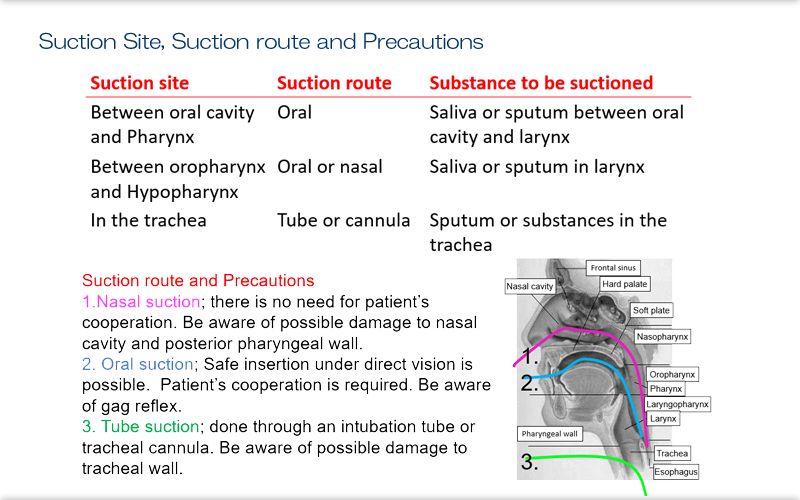
This is a diagram of a suction passage.
When performing endotracheal suctioning, check the length of tube in advance to make sure that it doesn't reach the tracheal bifurcation. Beginners should suction inside the endotracheal tube only, and they should switch with an experienced practitioner if deeper suctioning seems necessary.
Explanation
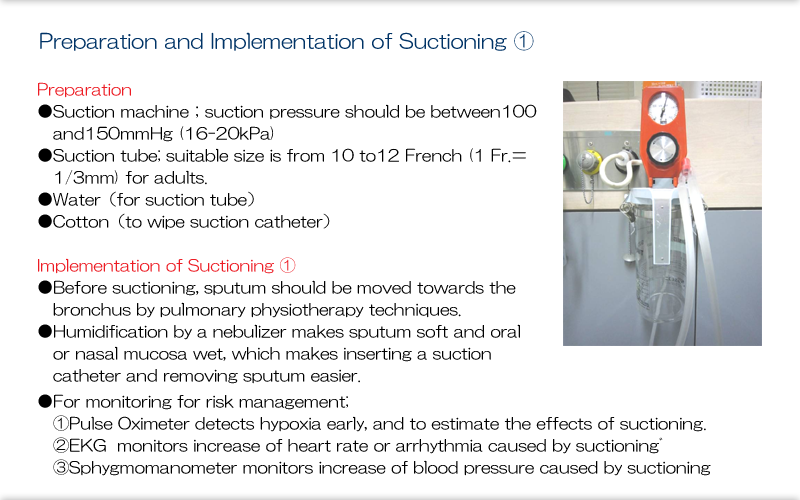
This is a typical outlet-type suction machine. If you bend the suction tube to block the flow of air and turn the black dial to the right, the pressure gauge moves and pressure increases. While keeping the tube bent, adjust the pressure to the appropriate level.
You should know in advance about the design of the suction catheter you will use. Almost all have holes in the tip and sides. They also have an air hole where the catheter is held, and uncovering this hole stops suction pressure from reaching the tip. When inserting the catheter, uncover the hole to ensure no suction pressure is applied. Once you reach the target area, cover the air hole with a finger to start suctioning.
If the catheter does not have this hole, you can bend the central part with your finger to block off the central part.
When you begin suctioning, air will be drawn down into the airway, which will reduce breathing. Various reactions to this change, as well as mechanical stimulation of the larynx, may cause events such as a vagal response, so it is best to monitor the patient during the procedure.
Explanation
Suctioning must be performed with care.
Excessive suction pressure can cause the catheter to adhere to the mucosa and injure it.
Suctioning sessions must be limited to 10 seconds. Longer suctioning may impair ventilation.
There are no major complications for non-endotracheal suctioning.
Endotracheal suctioning can cause complications like those shown here.
The following procedures for handling complications are taken from the Guidelines for Endotracheal Suctioning.
Procedures for handling complications: If the complications mentioned above occur during suctioning or you think that anything might be wrong, stop suctioning immediately and make an assessment. Watch the percutaneous oxygen saturation monitor. If it shows circulatory insufficiency (eg, hypoxemia or arrhythmia), administer 100% oxygen and immediately call for another person (a colleague or doctor). **Explanation: Major causes of arrhythmia and bradycardia are hypoxemia, myocardial hypoxia, and vagal response triggered by airway stimulation. Coughing induced by airway stimulation increases airway pressure, which reduces venous circulation and cardiac output. It is important to have a system in place to ensure that a doctor can quickly assist in an emergency. Tracheal suctioning should be performed under a medical control system. Essentially, this means that a system must be in place that ensures that doctors can reliably give instructions and provide treatment in an emergency, whether it occurs inside or outside the hospital. In the event of cardiac arrest, the worst complication that can occur, cardiopulmonary resuscitation must be performed immediately. This is why anyone who performs tracheal suctioning should take a class on basic cardiopulmonary resuscitation and learn those skills.