Explanation
Videofluorography examination of swallowing (VF) can visualize movements involved in swallowing and managing a food bolus, which can't be observed externally. Thus, VF is very useful for identifying the cause of dysphagia and determining treatment strategy. However, the lack of a standardized procedure often leads to inaccurate evaluation. This module describes the standard procedure for, and complications associated with, VF and its management.
Explanation
We need to explain to our patients the purpose and actual procedure of the examination so that they can understand and consent to the examination. Telling them that the safety of eating can be assessed by this examination can ease their concerns about undergoing VF.
Whenever possible, patients who have not eaten orally for a long time should receive indirect exercise before undergoing VF.
Performing VF in patients who are nervous in the examination room is likely to result in inaccurate evaluation and is also associated with increased risk of aspiration. So, it is advisable for examiners and patients to get to know each other before the examination, and patients should do light warm-up exercise to relax tension in the neck and shoulder muscles.
Explanation
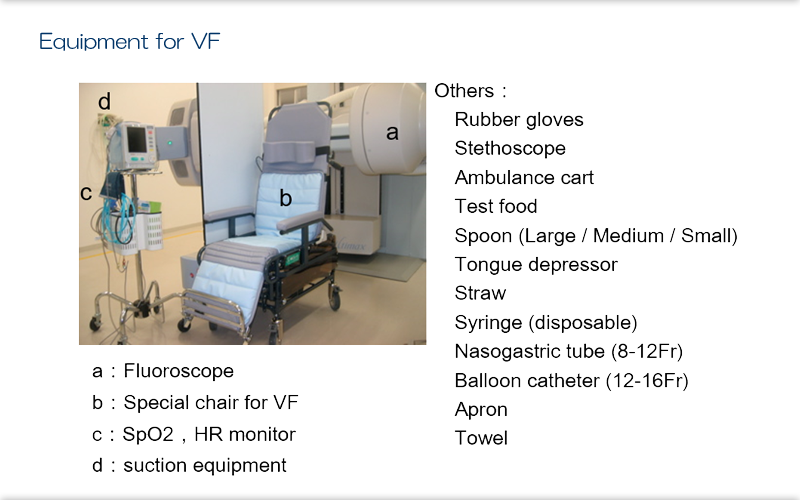
Although VF is a safe examination, it is advisable to monitor pulse rate and percutaneous oxygen saturation during the examination.
An suction equipment should be made ready to use in case of aspiration or pharyngeal pooling.
As an infection control measure, examiners should use a new set of gloves for each patient.
Test foods should be prepared in advance with sufficient consideration of the purpose of the examination.
Also, nasogastric tubes and balloon catheters should also be made ready for immediate use.
Explanation
The etiology of dysphagia and whether or not the condition is treatable affect the examination procedure, so they should be determined before the examination.
Patients with a history of aspiration pneumonia and those who have long been NPOs need special attention because of the high risk of aspiration. Examiners should fully understand the purpose of each examination as requested by the referrer for VF (eg, attending physician or attending trainer) to ensure a proper examination.
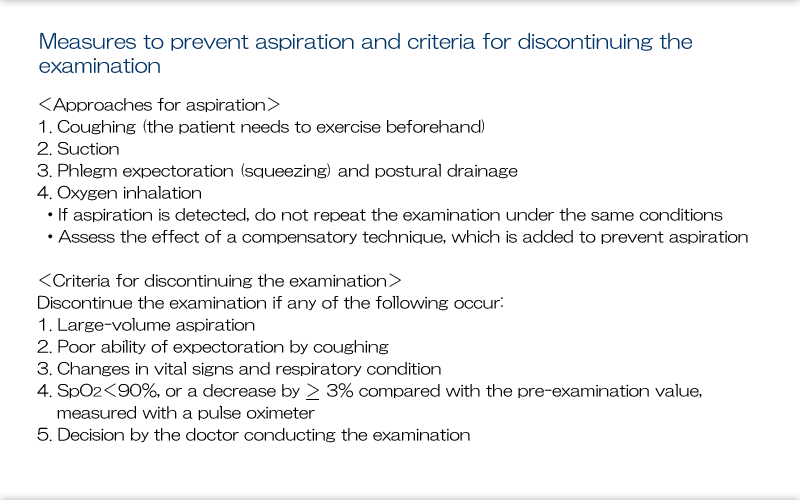
Examinations should be discontinued if patients experience disturbed consciousness or have a poor general condition on the day of the examination.
Thorough oral care should be done prior to the examination. If patients have extremely poor oral hygiene on the day of examination, discontinue the examination or give oral hygiene first before examination.
Explanation
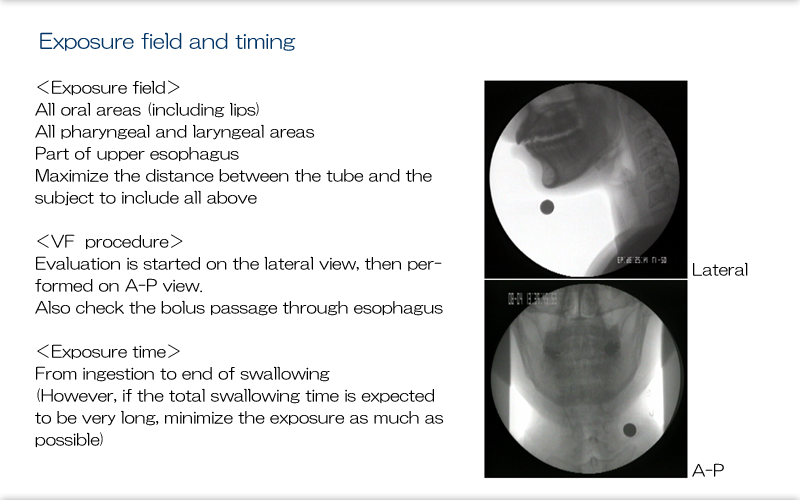
Adjust the irradiation field to include all of the oral cavity, pharynx, and larynx. Ensuring a sufficient distance between the tube and the area to be visualized will reduce the magnification needed of the area and provide a sufficient irradiation field and clearer images.
Start with lateral projection and then move to anteroposterior projection. During this procedure, evaluate middle and lower esophageal peristalsis and whether there is any residual material.
Irradiation should start when the food bolus is captured by the mouth and should end when the swallowing reflex is completed and the larynx returns to the resting position. When there is no swallowing reflex, irradiation should be interrupted until the swallowing reflex is stimulated by verbal instruction or swallowing maneuvers.
Total irradiation time should preferably not exceed 5 min.
Explanation
During the examination, posture should be the same as that during daily eating.
For patients who have not eaten orally for a long time, initially place them in a 30° elevated supine position with the neck bent forward and then gradually increase the angle while ensuring safety. Also, ask patients to dry swallow before starting VF and if there is any impairment of pharyngeal contraction, laryngeal elevation, or laryngeal closure and aspiration is likely to occur in a sitting upright position, adjust to a reclined position.

Explanation
A nasogastric tube can interfere with swallowing movement depending on its thickness and course, and it should be removed before the examination to ensure optimal assessment of swallowing.
When direct training needs to be done with a nasogastric tube in place, the tube should not be removed because the assessment of eating safely needs to be done taking into account the effect of the tube. When the tube has to be removed during the examination, it is advisable to re-insert a new tube with appropriate thickness and check the course and depth of the new tube under fluoroscopy.
Explanation
For patients with an uncuffed tracheostomy tube, it is advisable to perform the examination with the speech valve and the stopper in place. So, determine whether the valve and stopper can be closed before the examination.
For patients with a cuffed tracheostomy tube, remove secretions accumulated over the cuff by suctioning before the examination.
Also, before the examination, make sure that deflating the cuff does not result in breathing difficulties or reduces SpO2 and check whether the speech valve and the stopper can be placed. If possible, evaluate swallowing function with the speech valve and stopper in place.
Explanation
At the initial examination, assess the movements of the oral cavity, tongue, pharynx, and larynx during phonation and dry coughing without using a contrast agent. Then, using a contrast agent, perform a rough examination in lateral and anteroposterior projections and then make a detailed examination again in lateral projection using compensatory maneuvers. In anteroposterior projection, assess the laterality of pharyngeal contraction and bolus passage through pharynx and UES, as well as esophageal peristalsis and residue.
This does not apply when re-evaluating specific compensatory techniques in the subsequent sessions.
Explanation
To minimize the risk of aspiration, it is important to start with a safer examination and gradually increase the level of diffivulty of the examination. Change one factor, not multiple factors, at a time-such as first changing the physical properties of the food, then the amount in a mouthful, and finally posture-and evaluate the effect of changing each factor.
Explanation
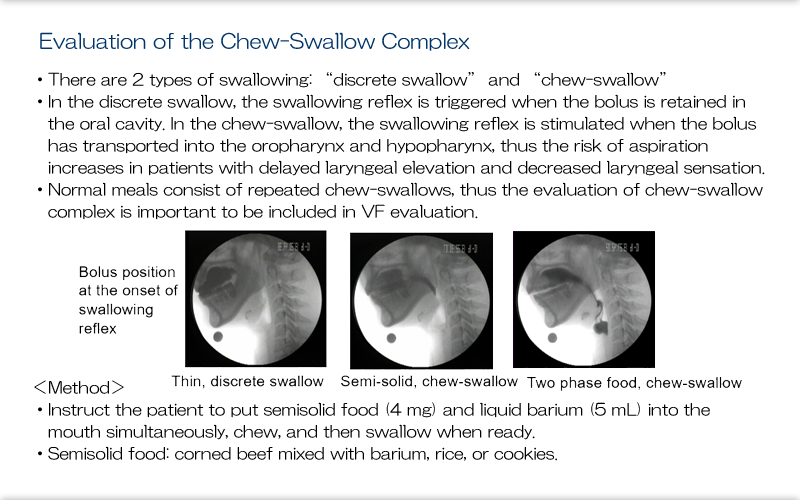
A discrete swallow and the chew-swallow are totally different in terms of kinetics. To minimize the discrepancy between daily eating behavior and VF findings, it is advisable to include the evaluation of chew-swallow in VF. The standard procedure is to instruct the patient to put 4 mg of semisolid food (corned beef kneaded with barium) and 5 cc of liquid barium into the mouth simultaneously and chew and swallow them1,2. Semisolid food can be substituted by rice or cookies. This test evaluates the bolus position at the onset of swallowing reflex and the presence or absence of aspiration during the course of thorough processing and swallowing.
Explanation
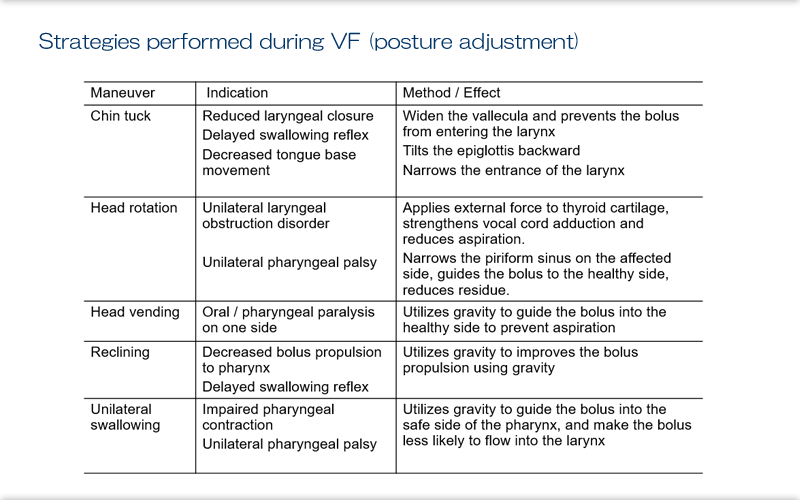
Here we see the postural adjustment that can be used as compensatory techniques during the examination.
These methods should be combined with voluntary swallowing maneuvers (described on the next slide) to explore the optimal swallowing method which is least likely to cause aspiration and pharyngeal pooling
Explanation
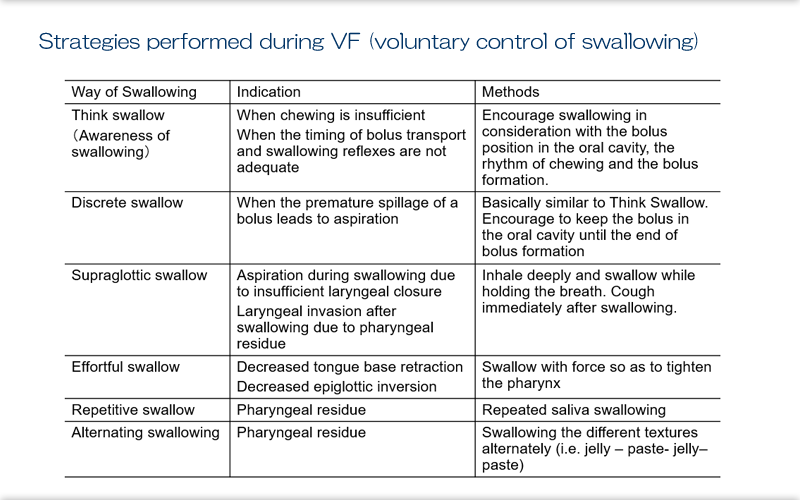
Here we see voluntary swallowing strategies that can be used as compensatory techniques during the examination. Evaluate the effect of each maneuvers and utilize them in the direct exercise and the daily meal.
Explanation
When aspiration is detected, take appropriate approaches to deal with aspiration, rather than discontinuing the examination immediately. If there is no impact on the patient's general condition, consider whether there is any compensatory maneuver that can prevent aspiration.
Do not resume the examination under the same condition that caused the aspiration. Coughing force plays an important role in the expectoration of aspirated material and can be augmented by breathing and coughing training as part of physical therapy before the examination. Postural sputum drainage is also effective for massive aspiration.
Explanation
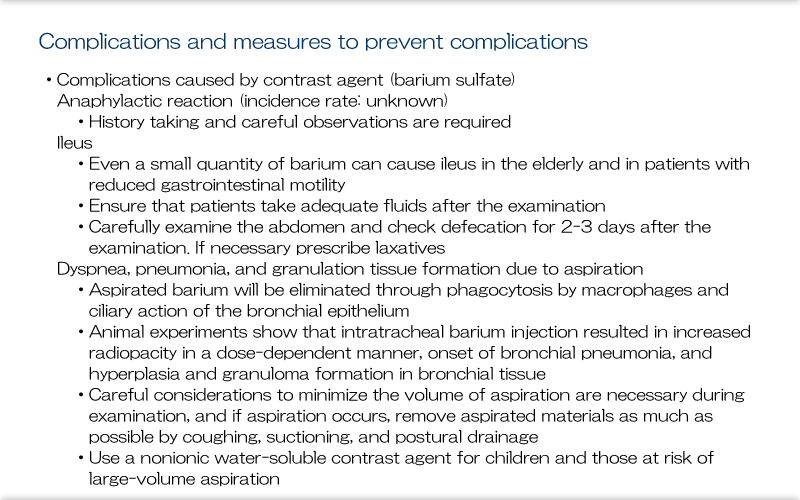
Common complications of VF include those caused by contrast agents.
Barium sulfate is a commonly used contrast agent and is considered to cause minimal harm to humans due to its water insolubility. However, it has been associated with the risk of ileus in the elderly and in individuals with reduced gastrointestinal motility3, and it can cause pneumonia and granulation tissue formation when a large volume is aspirated4. Careful monitoring and examination is needed to manage these risks. For patients considered to be at risk of massive aspiration and for children, consider using a water soluble, nonionic contrast agent to ensure a minimally invasive examination.
References
- Takeda S, Saitoh E, Matsuo K, Baba M, Fujii W, Jeffery B PALMER:Influence of Chewing on Food Transport and Swallowing, J Rehabil Med, 39(6):322-330, 2002
- Yokoyama M:Evaluation of the Chew-Swallow Complex, Modern Physician, 26(1):42-45,2006
- Tagami K, et al:Surgery, 52(4), 410-411, 1990
- Wada K, et al:JSGE, 79(10), 2035, 1982