Explanation
Training for patients with dysphagia requires guidance on safe and effective oral eating. This module explains the concept behind step by step swallowing training and the procedures used.
Aims of this module are;
1)to explain the concept behind step by step swallowing training
2)to explain the eligibility for step by step swallowing training
3)to explain the procedures used in step by step swallowing training
4)to explain the important points to observe and cautions when performing this training
Explanation
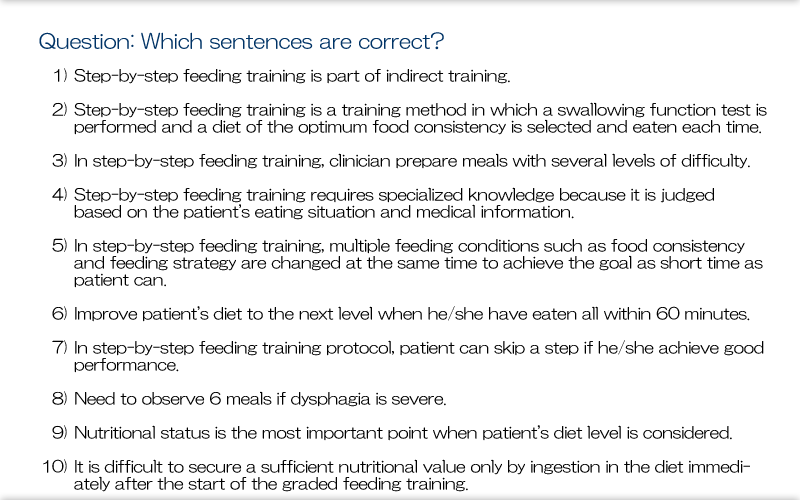
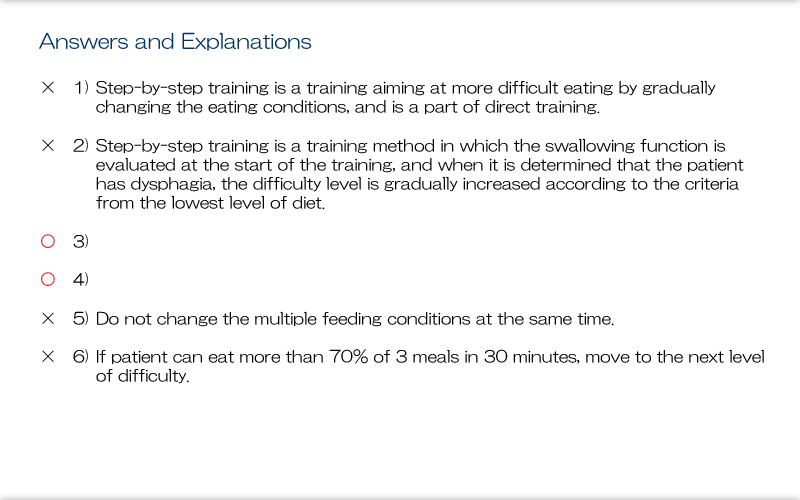
Step by step feeding training starts with a low degree of difficulty and proceeds with increasing degrees of difficulty, with the ultimate aim of achieving normal oral eating with a normal diet in a sitting position. This form of training involves eating actual food, so we need to fully consider risk management. Step-by-step feeding training targets patients with dysphagia. It is also been used to enable safe and effective oral eating in all age groups, from children to the elderly, after prolonged periods of non-oral eating. In such cases, an understanding of step by step swallowing training can provide a reference for the approach we should take.
Explanation
Graded swallowing training involves postural adjustment and setting the diet, method, and pace for oral eating as well as the mouthful size. These intake conditions are then changed in small steps. Observation during graded swallowing training crucially focus on confirming safety. In graded swallowing training, we need to use a type of food that matches the degree of difficulty at each step and ensure such food is available for training sessions. So, we need to choose food for each step and create a menu in cooperation with rehabilitation specialists and other health professionals involved in the graded swallowing training, especially specialists in cooking and nutrition. For the type of food to be used at each step, refer to the Japanese Society of Dysphagia Rehabilitation's "Japanese Dysphagia Diets 2013". With graded swallowing training, we judge that patients can progress to the next step based on medical observations and observations and grading of oral eating ability. Accordingly, specialist knowledge is needed to properly observe the dysphagia and general condition. The following are important when providing graded swallowing training: regularly reviewing the food prepared from the standpoints of food preparation and use in the swallowing training, and ensuring the availability of such food every day. Also, we have to establish the conditions in which oral eating can occur and the clinical observations to be made and recorded.
Explanation
The following patients are eligible for graded feeding training:
Dysphagia Patients who are necessary to do the training for acquiring the new skills of eating after evaluating the posture, oral eating methods, and food type.; those with dysphagia who are expected to show some improvement with graded swallowing training; and those who have not eaten orally over the long term (including all age groups from children to the elderly). Graded swallowing training involves making small incremental changes in oral eating conditions based on clinical observations, and patient eligibility requires that safe oral eating is an achievable goal.
Explanation
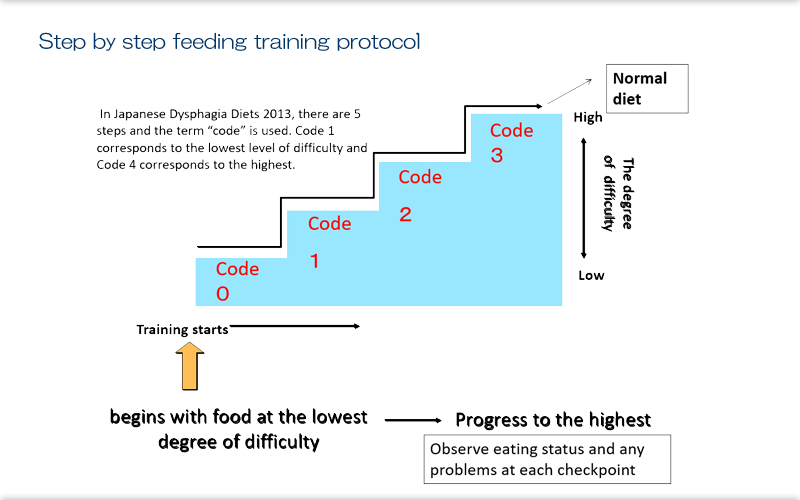
Graded feeding training is like climbing stairs one step a time, with the degree of difficulty increasing as we ascend. Currently, in Japan, we have many centers that can provide training for steps 3 to 5. In Japanese Dysphagia Diets 2013, there are 5 steps and the term "code" is used. Code 1 corresponds to the lowest degree of difficulty and Code 4 corresponds to the highest. Standard graded swallowing training begins with food at the lowest degree of difficulty and progress from there. Training involves using oral eating methods and posture that prevent aspiration as far as possible. Patients continue training under the same conditions for a fixed period, and their eating status is checked to see if any issues emerge. If no issues then emerge, the patient can ascend one step, and is observed again in the same way. This process is repeated increasing the degree of difficulty step by step. Ultimately, the aim is for the patient to consume a normal diet. Determinations on increasing the degree of difficulty are based on the standards for level of diet stated below, with observations of eating status and any problems at each checkpoint.
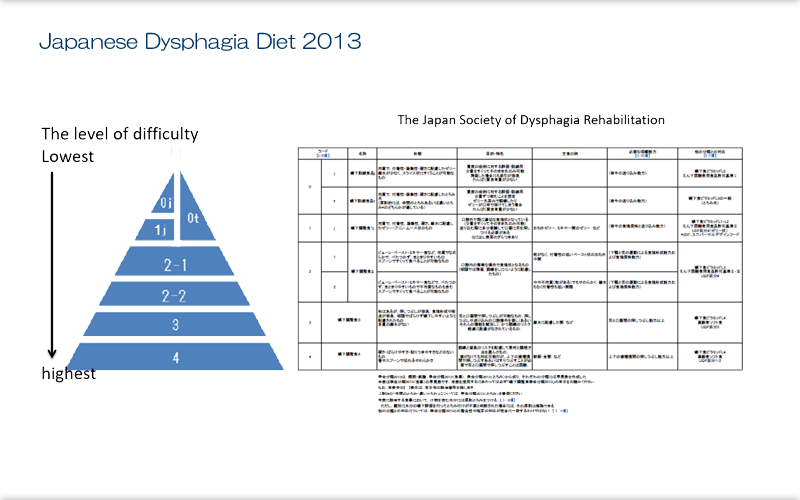
Explanation
The Japan Society of Dysphagia Rehabilitation's Japanese Dysphagia Diets 2013 presents a representative example of graded swallowing training and highlights the need for a precise classification of food texture for rehabilitation, starting from easy-to-eat food to a normal diet. Japanese Dysphagia Diets 2013 uses a 5-step classification, from Code 0 to Code 4. Because patients with a range of diseases can need a modified dysphagia diet, foods at the lowest degree of difficulty are currently further classified with "j" for jelly-type food or "t" (for thickened food)[[OK as added to improve logical flow?]]. Also, to prevent abrupt decreases in the degree of difficulty, Code 2 is divided into two subcategories, Codes 2-1 and 2-2.
Explanation
We raise the level of difficulty in graded swallowing training initially in relation to the consistency of the food and the amount eaten. Normally, we change consistency and amount at the same time as patients move to the next step in eating. When patients are ready to move on a step with a certain food, we must then consider the frequency of eating, whether eating will be assisted or independent, what oral eating method will be used (technique, posture, and mouthful size), and when the next step will start. However, as the training step changes, we should not make changes to multiple items at this time. Changes in eating conditions are associated with the risk of aspiration, and if this occurs then we can quickly identify and manage the problem when only one condition has been changed. Generally, frequency is set at 3 meals per day from step 2 (ie, Code 2), but it can stay at 1-2 meals per day, depending on the patient's condition.
Explanation
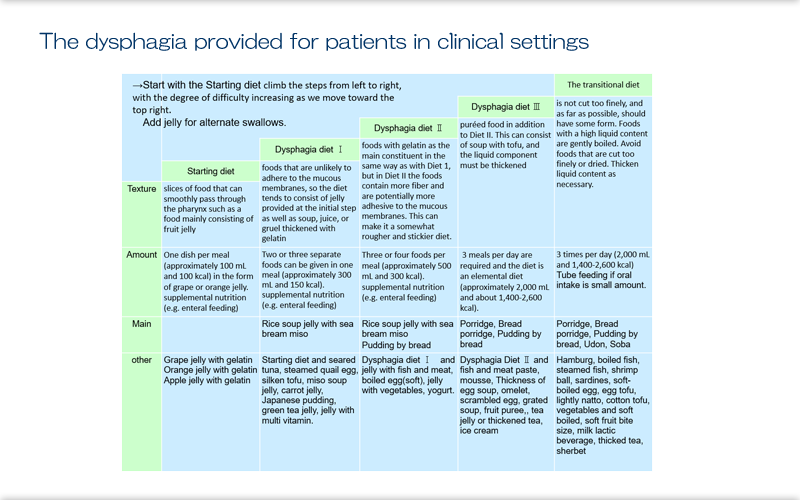
Here we see the diets provided for patients in clinical settings. These are standard diets used in graded swallowing training, and the training is provided based on these standard diets. They start with slices of food that can smoothly pass through the pharynx such as a food mainly consisting of fruit jelly. This constitutes one dish per meal (approximately 100 mL and 100 kcal) in the form of grape or orange jelly.
In Swallowing Diet I, patients are given foods that are unlikely to adhere to the mucous membranes, so the diet tends to consist of jelly provided at the initial step as well as soup, juice, or gruel thickened with gelatin. Two or three separate foods can be given in one meal (approximately 300 mL and 150 kcal).
In Diet II, patients are given foods with gelatin as the main constituent in the same way as with Diet 1, but in Diet II the foods contain more fiber and are potentially more adhesive to the mucous membranes. This can make it a somewhat rougher and stickier diet. Patients are given 3-4 foods per meal (approximately 500 mL and 300 kcal).
In Diet III, patients are given puréed food in addition to Diet II. This can consist of soup with tofu, and the liquid component must be thickened. At this step, 3 meals per day are required and the diet is an elemental diet (approximately 2,000 mL and about 1,400-2,600 kcal).
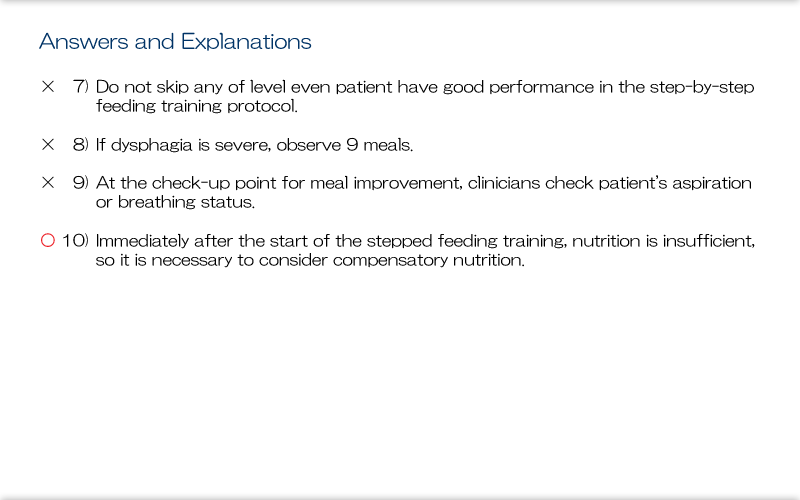
The transitional diet is not cut too finely, and as far as possible, should have some form. Foods with a high liquid content are gently boiled. Avoid foods that are cut too finely or dried. Thicken liquid content as necessary. This is also an elemental diet provided 3 times per day (2,000 mL and 1,400-2,600 kcal), similar to Diet III. Having Diet III and the transitional diet meets daily nutritional requirements; depending on the amount of oral intake, supplemental nutrition may be continued via, for example, enteral feeding. Diet I and Diet II are each provided with supplemental nutrition via, for example, enteral feeding because these diets don't provide sufficient nutrition in themselves. The variety of foods is increased as the patients advance through the steps. Commercially available nursing care foods, some of which are sold in supermarkets, can be used from the initial step. The ingredients may be chosen depending on the stage or they may need to be altered to adjust the food texture.

Explanation
Here we see a photograph of actual diets. We climb the steps from left to right, with the degree of difficulty increasing as we move toward the top right. When there is to be jump in the degree of difficulty between steps in training, an additional set of foods may be added in the transition between the steps. Some medical centers determine food texture on their own.
Explanation
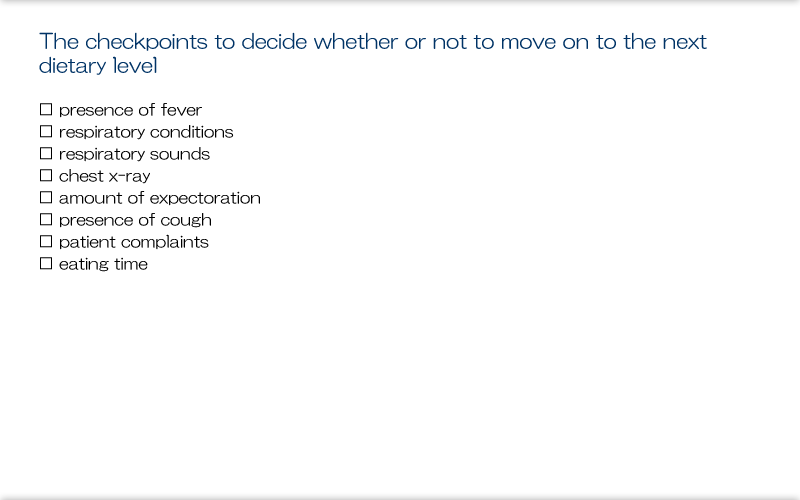
To be able to move to the next step in the diet, patients must be able to eat 70% of the meal provided within 30 min for 3 consecutive meals. The 3 meals represent a checkpoint (see below) where we should observe them eating, and we can move to the next dietary step only when they show no clear abnormalities. For severely dysphagic patients, it is recommended that they be observed for 9 mealtimes (over 3 days).
Explanation
The presence or absence of aspiration is the main finding determined at the checkpoint to decide whether or not to move on to the next dietary step. Other parameters assessed include fever, respiratory condition, respiratory noise, chest X-ray, expectoration, coughing, patient complaints, and eating time. If there are any abnormalities in any of these parameters at a certain dietary step, then we must not move the patient on to the next dietary step, and we need to investigate the cause of the abnormality.
Explanation
Graded swallowing training is a training procedure where the degree of difficulty in oral eating conditions is increased incrementally in steps. In actual clinical settings, the key to success in this training is to observe patients in detail. If patients with dysphagia show any problem, such as reporting not eating well when there is a slight change in food texture or change in their physical condition, we need to take a more detailed tailored approach for them.
To sum up the main points so far,graded swallowing training involves a stepwise increase in the degree of difficult in oral eating. Therefore, increasing the degree of difficulty needs to be done in small steps. For example, the diet for oral eating is increased one step at a time, and steps must not be skipped.
Furthermore, during the training, we need to confirm that the food being given to patients retains the texture specified in their diet when it was initially prepared. Its texture may alter between preparation and eating or food components separate out, especially liquids. In particular, gelatin melts at ≥ 18ºC, so we need to consider the time between the food being prepared and eaten. The texture of rice porridge may change due to changes in temperature or the liquid can separate out. Characteristically, rice porridge becomes stickier at low temperatures when placed in a food blender. As we can see then, training should be provided with an understanding of the texture of the relevant diet.
At the same time, we also need to ensure that a system is in place where food with the same texture is provided on a daily basis. Differences in texture can occur with different preparation methods, so we need to consider such factors as the heating process and its duration as well as providing food with the same texture for graded swallowing training.
Adjusting the texture is also vital in graded swallowing training. We need to check that the texture of the food prepared for training (eg, jelly or pureed food) is suitable for the training. Sometimes soft foods are provided with jelly and pureed food, and all of the food should be examined for both texture and form.
When patients are transitioning to the next step and we are not sure if the transition will be smooth, it is fine to try giving them one food from the diet in the next step. The transition can then be made adding one more food at a time until finally reaching the full diet for that step; with this process, the graded training can be done in smaller steps.
When patients move on a step, the earliest possible time to assess whether the transition has gone smoothly is after 3 meals.
As we noted earlier, conditions for oral eating are changed by increasing the degree of difficulty one step at a time and not by changing multiple conditions at the same time. When deciding which condition to change next, we need to ensure that information is shared between the patient, their family, and medical staff at that time and that the decision is made after thorough discussions.
Explanation
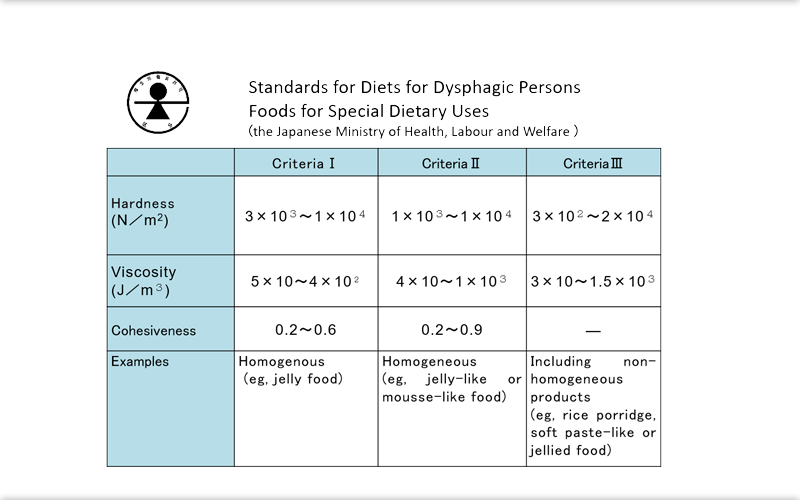
The grading of dysphagia diets in Japan is standardized and aims at consistency in training. If we can achieve this consistency, we will be able to provide significant support for dysphagic patients in their daily life and will importantly allow them to continue receiving training after discharge or transfer to another hospital. In 2009, the Japanese Ministry of Health, Labour and Welfare stipulated the "Licensing Standards for Diets for Dysphagic Persons"[[We couldn't find any official English]] in "Foods for Special Dietary Uses" with a 3-step classification system. These standards subsequently fell under the remit of the Consumer Affairs Agency and current food labeling standards. Under these standards, foods are classified as "hard", "agglutinative", or "sticky". These standards were established for patients with relatively severe dysphagia.
Explanation
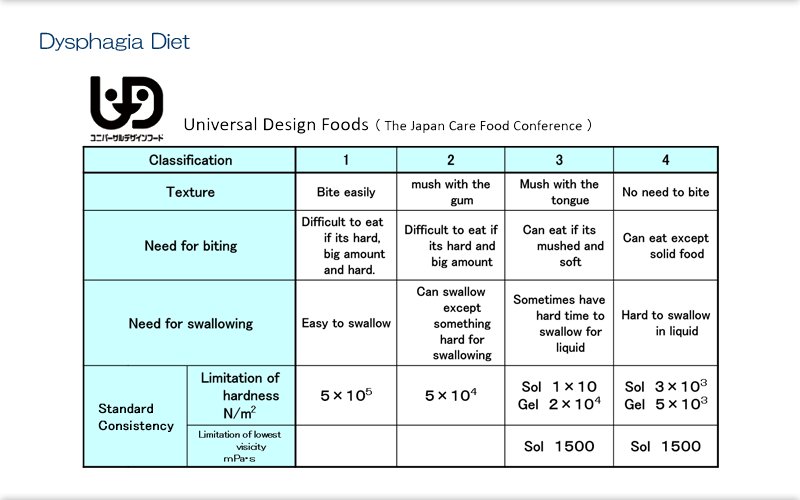
The Japan Care Food Conference drew up standards with 4 stages, the "Universal Design Foods". These standards were developed to cover mastication. They classify biting strength and swallowing strength as well as apply standards of hardness and viscosity. These standards were established for patients with more capability than the other standards.
Explanation
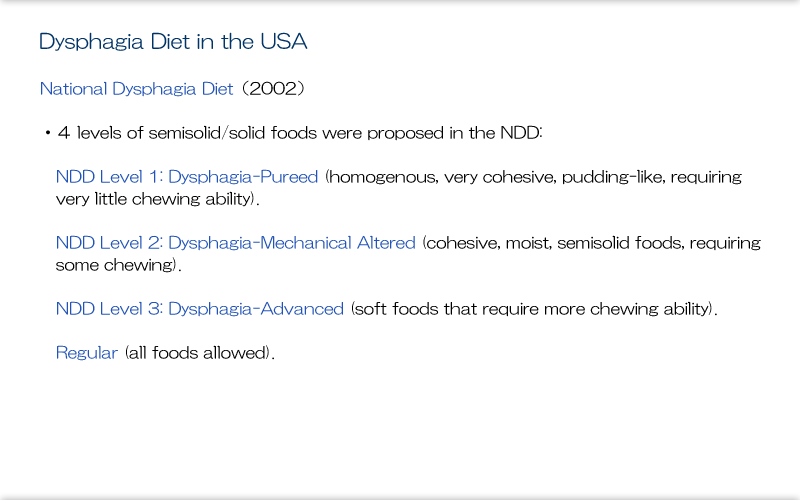
Here we see the standard called the National Dysphagia Diet, which was developed in the United States in 2002. It has 4 levels, with the top level indicating a regular diet. This diet differs from its Japanese equivalent in that the food with lowest degree of difficulty is puree. Gelatin is widely used as a food for swallowing training in Japan but not in America. At Serei Mikatahara General Hospital, our standard practice is to start patients somewhere between swallowing Diets II and III. National Dysphagia Diet were established for milder cases of dysphagia compared with the Japanese dysphagia diet standards.
Explanation
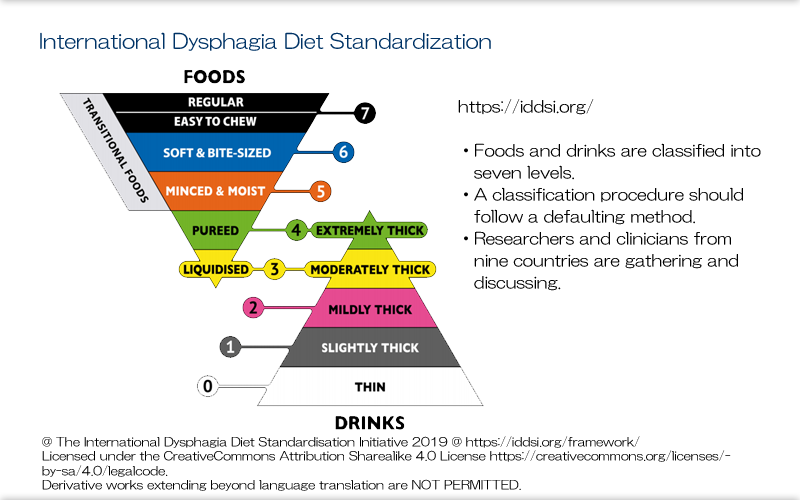
Recently, there have been moves to standardize dysphagia diets internationally. Experts from around the world, including North America, Europe, and Japan, have been meeting to discuss such standardization. With this movement, graded swallowing training may be entering an age where is it provided in the same way globally.
References & Recommended reading
- Fujishima I & Taniguchi H:Rehabilitation for Swallowing Disorders associated with Stroke, 3rd edition. Ihiyaku Publishers 2017
- Saitoh E & Ueda K eds:Dysphagia Rehabilitation, 3rd edition. Ihiyaku Publishers 2016
- Seirei Mikatahara General Hospital Swallowing Team eds: Pocket Manual of Dysphagia, 4th edition. Ishiyaku Publishers, 2018
- Kurachi M ed: Dysphagia Textbook for Speech-Language-Hearing-Therapist. Ishiyaku Publishers, 2013