Explanation
In severe cases of dysphasia that don't improve with rehabilitation, otorhinolaryngologists sometimes perform surgical treatment. The techniques we use are divided largely into two: surgeries to improve swallowing function and surgeries to prevent aspiration. In this module, we look at the surgical treatment options available.
Explanation
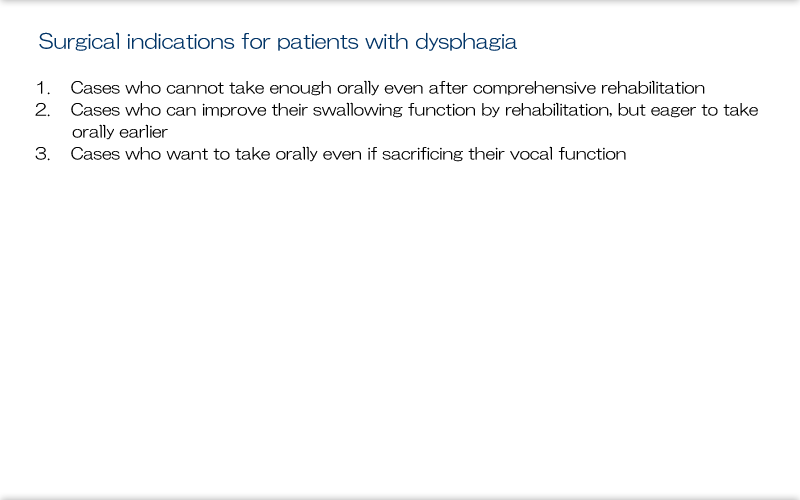
First, in relation to indications for surgery, we have to consider the following.
1) Even with general rehabilitation programs, improvement can level off in about half a year. When adequate oral eating can't be achieved at that point, we should consider the need for surgical treatment. With long-term rehabilitation, patients can lose motivation and with disuse, even when surgery is performed, adequate treatment effects are often not obtained because of surrounding muscle weakness.
2) Many patients are treated with rehabilitation, but surgical treatment can help certain patients re-integrate into society quicker than they would by achieving oral eating by rehabilitation alone. So, when deciding on the treatment plan, we must evaluate the need for surgical treatment and maintain communication with otorhinolaryngologists.
3) In neuromuscular or degenerative disease, for patients whose swallowing function is expected to decrease over time despite receiving aggressive rehabilitation or for patients with severe impairment in whom aspiration pneumonia will recur despite being NPO, we can perform surgical techniques that separate the trachea and esophagus and sacrifice vocal function in order to preserve life.
Explanation
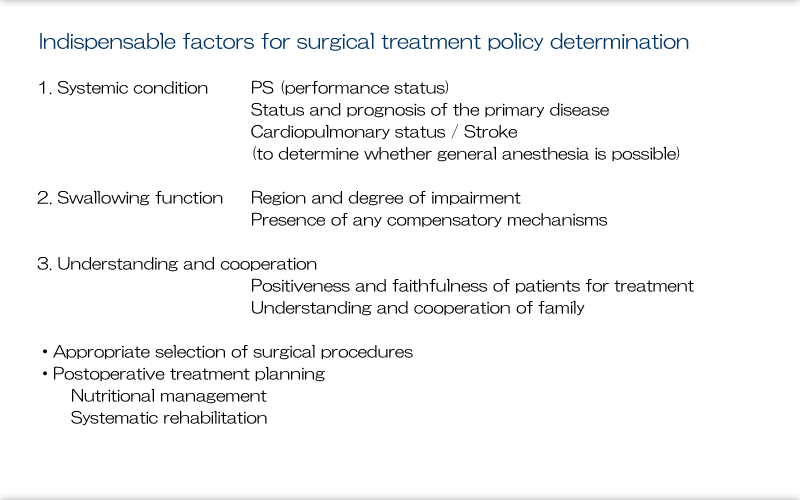
When considering surgical treatment, we need to make certain evaluations. First, to understand overall status, It's important to begin with determining performance status (PS), the status and outcome of the primary disease, and cardiopulmonary status to determine whether general anesthesia is possible. Next, obviously we need to evaluate swallowing function. Of note, PS is an indicator of how active patients may be. On a 5-point scale from 0 to 4, 0 indicates there are no symptoms, so social activity is possible, 1 indicates has difficulty with physical work, 2 indicates is ambulatory but has difficulty with light tasks, 3 indicates requires assistance with daily activities and is bedbound over 50% of the time, and 5 indicates completely bedbound.
We need to closely evaluate the findings of swallowing contrast imaging and examine the region and degree of impairment, the presence of any compensatory mechanisms, and the presence of silent aspiration during unintentional swallowing. As a final point, it is important to consider the issue of the patients themselves and their families. Because surgical treatment has some degree of invasiveness, this cannot begin without the understanding of, and cooperation with, treatment from the patients and their families.
Explanation
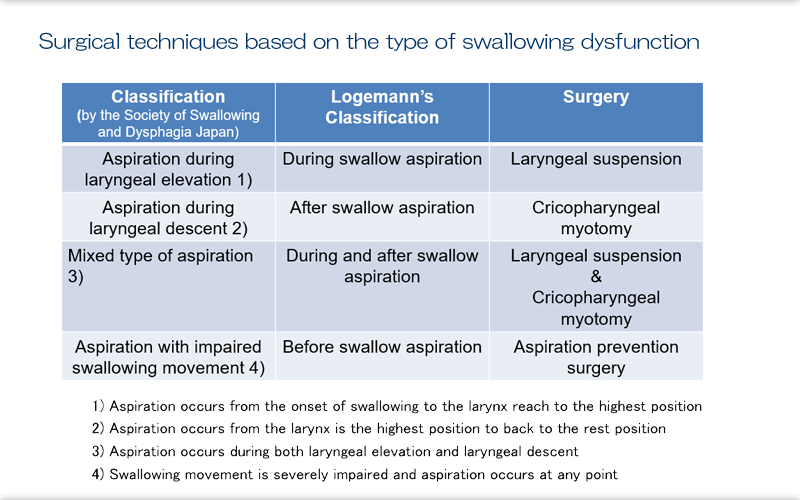
In reality, the effectiveness of a single surgery is low, and several surgeries are usually performed, and this shows the correlation between the surgical techniques and the impaired region identified by videofluoroscopy on the basis of which the surgical technique is selected. We can opt for laryngeal suspension to treat aspiration during laryngeal elevation (during swallow aspiration), cricopharyngeal myotomy for aspiration during laryngeal descent (after swallow aspiration), and procedures to prevent aspiration for aspiration with impaired swallowing movement (before swallow aspiration).
Explanation
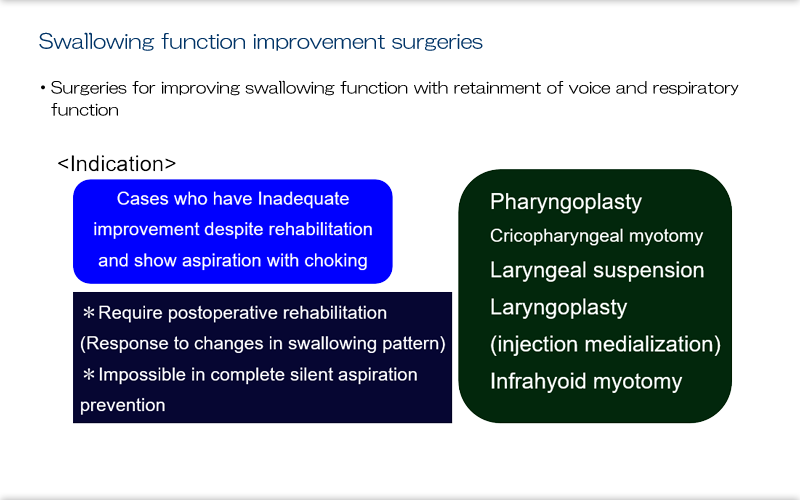
Surgeries for improving swallowing function are surgeries that retain swallowing function while preserving the vocal and respiratory function of the larynx. The indication for such procedures are inadequate improvement despite rehabilitation for aspiration with choking. There are many techniques we can perform, including pharyngoplasty, cricopharyngeal myotomy, laryngeal suspension, laryngoplasty (injection medialization), and infrahyoid myotomy. But the important thing is that the position of the larynx changes due to surgery, and this requires postoperative rehabilitation, which is contraindicated in patients with marked silent aspiration.
Explanation
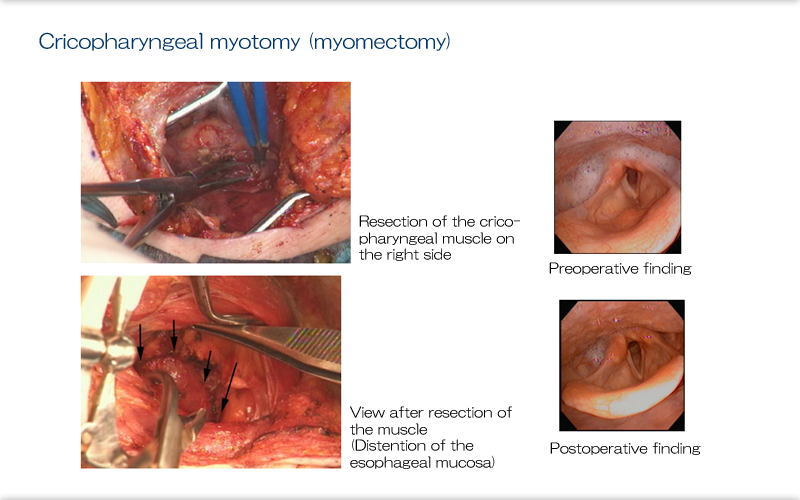
A representative surgery for improving swallowing function, cricopharyngeal myotomy, as seen in the operative photo, is a technique with a cervical incision where the bilateral cricopharyngeal muscles are adequately excised until the esophageal membrane is exposed. We opt for this when the cricopharyngeal muscles, which relax only during swallowing, aren't adequately relaxed during swallowing due to bulbar paralysis. Postoperative laryngeal examination with a fiberscope revealed that the preoperative pooling of saliva in the bilateral piriform sinus was gone due to adequate relaxation of the esophageal orifice following resection of the cricopharyngeal muscles.
Explanation
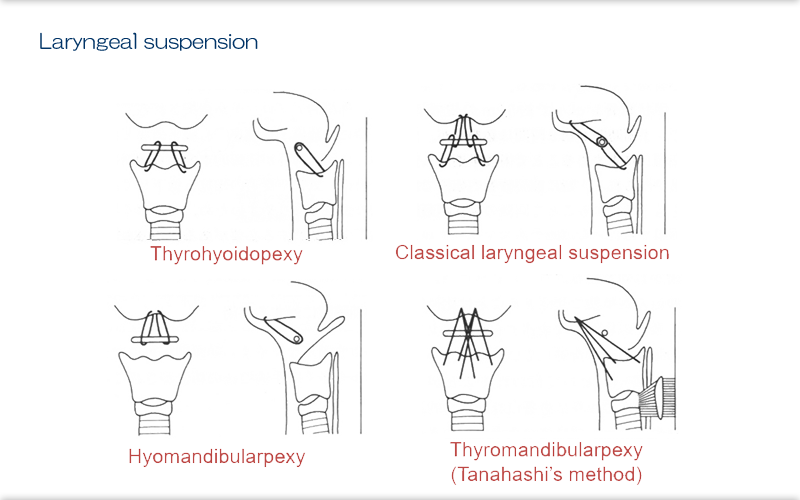
The other surgical technique that is important in surgeries that improve swallowing function is laryngeal suspension. Depending on the position and direction of elevation of the thyroid cartilage which houses the larynx, there are 4 methods to choose from. We can opt for thyrohyoidopexy to assist upward elevation of the larynx, hyoid advancement to the mandible to supplement forward elevation, and thyrohyoid advancement or thyroid cartilage advancement when elevation is inadequate in the upward and forward directions.
Explanation
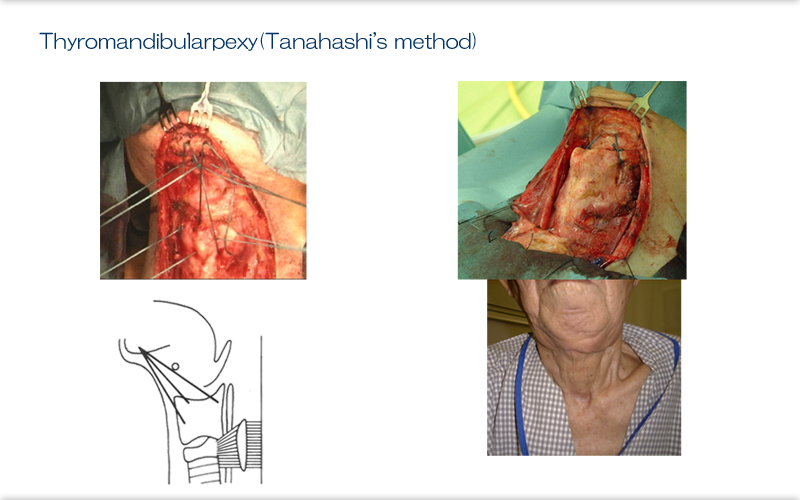
Also, for patients with the most severely impaired swallowing function, we may opt for a combined surgical technique involving thyromandibularpexy and bilateral cricopharyngeal myotomy along with temporary tracheotomy. This technique is called the Tanahashi's method after the surgeon who developed it and it enables voluntary opening of the upper esophagus by protruding the mandible.
Explanation
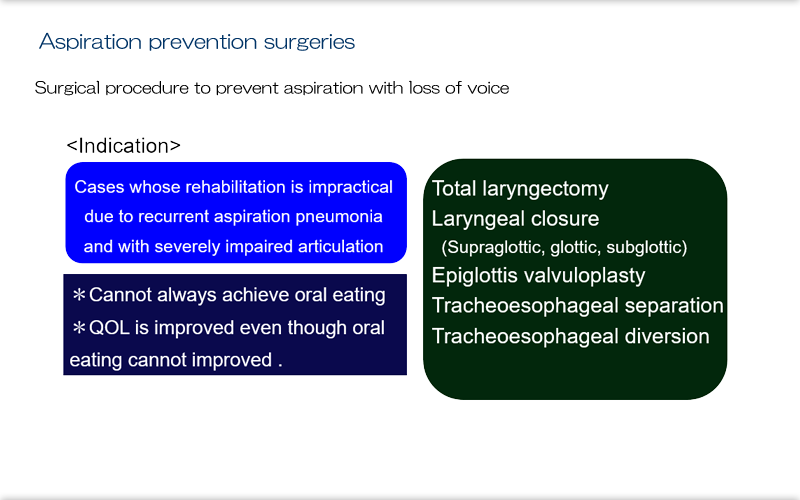
The second main surgical treatment for dysphagia is to prevent aspiration. In this surgery, vocal function is sacrificed. The surgery prevents aspiration pneumonia. The indications are rehabilitation that does not progress because of recurrent aspiration pneumonia and severely impaired articulatory function. The operative procedure starts with total laryngectomy, which is the previous standard treatment for advanced laryngeal cancer, and with various techniques such as laryngeal closure, epiglottis valvuloplasty, glottal closure, tracheoesophageal separation, and tracheoesophageal anastomosis; there are many variations. Most patients who undergo this procedure have poorer overall status preoperatively than patients undergoing surgery to improve swallowing function, so we need to do an evaluation of the whole body preoperatively. Also, because this surgery is only for prevention of aspiration, many patients who undergo it may not necessarily achieve oral eating, but in such cases QOL is still improved.
Explanation
Looking at the indications for surgery to prevent aspiration in a little more detail, we have severe silent aspiration (aspiration without choking) that is associated with pneumonia stemming from saliva aspiration despite being NPO, severely impaired articulatory function and a desire for oral eating and willingness to sacrifice vocal function, and degenerative disease or ALS with a desire for stable respiratory status using a ventilator.
Explanation
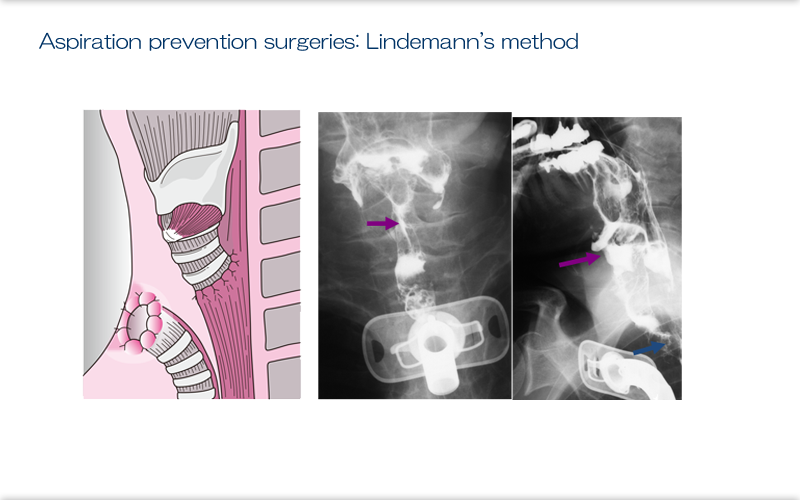
The Lindeman method has become the most widely performed surgical procedure for preventing aspiration in Japan. The cervical trachea is transected, a permanent tracheal stoma is constructed with the inferior stump, and the superior stump is anastomosed end-to-end with the cervical esophagus. The trachea and esophagus are completed separated, and even when there is subglottic aspiration, the bolus passes to the esophagus through the anastomosis. In cases where the esophagus is already resected and space for anastomosis to the esophagus can't be obtained, an alternative method uses the superior tracheal stump as a blind end. The point of this procedure, which sutures the superior and inferior trachea, is that it is reversible if swallowing function recovers along with the primary disease.
Explanation
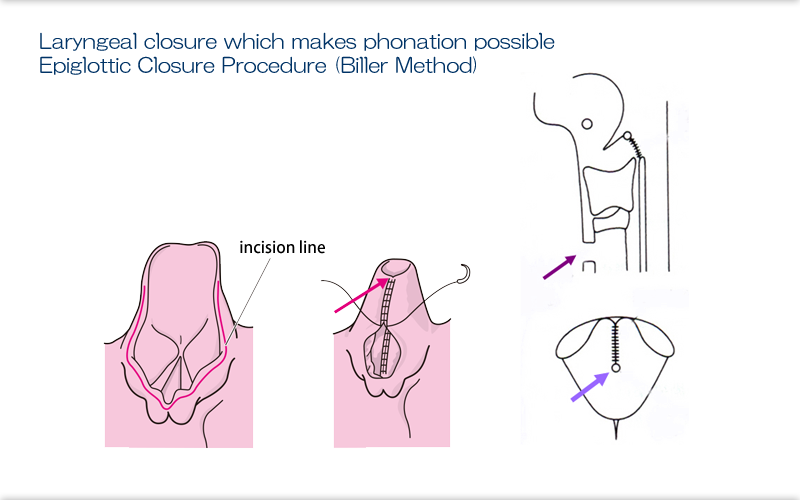
When patients wish to preserve even a little vocal function, we use the Biller method, or epiglottic closure procedure, to prevent aspiration. The membranes of the right and left epiglottic ends are sutured carefully in 2 layers and the tips alone are released, and careful handling is needed because the surgical field is somewhat limited and dehiscence may easily occur unless the elasticity of the epiglottic cartilage is adequately considered.
Explanation
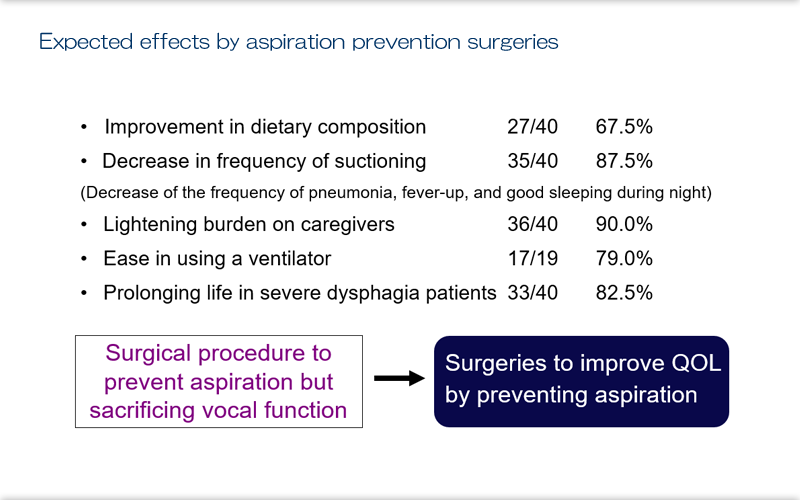
The outcomes of surgery to prevent aspiration, as noted from results shown, include improvement in dietary composition, significant decrease in frequency of suctioning, lightening burden on caregivers, ease of using a ventilator, and prolonging life in patients. Therefore, surgeries to prevent aspiration should be thought of not as surgery to achieve swallowing by sacrificing vocal function, but as surgery to improve QOL by preventing aspiration.
Explanation
While inevitably these surgeries are often thought of as irreversible last resorts simply because they are surgeries, there are many advantages: many can be reversed, they can resolve issues that can't be achieved quickly enough with rehabilitation, invasiveness is not so great, and, depending on the patients, the surgeries may be possible with local anesthesia. We otorhinolaryngologists view surgical treatment of dysphagia as one method to increase the effectiveness of comprehensive treatment.